Purpose of these Guidelines
The purpose of this chapter is threefold; 1) to identify the problem of mis-diagnosis of Schizophrenia in adults with trauma-based disorders originating in ritual abuse and trauma-based mind control (we will refer to these hereon as Ritual abuse/mind control traumatic stress), 2) to provide diagnosticians unfamiliar with the clinical presentation of Ritual abuse/mind control traumatic stress with guidelines to facilitate recognition of such cases and to thereby reduce the likelihood of their being mis-diagnosed as Schizophrenia, and 3) to provide diagnosticians experienced with Ritual abuse/mind control traumatic stress with guidelines to facilitate differential diagnosis between such trauma and Schizophrenia in cases with complex clinical features and diagnostic questions.
Mis-diagnosis results in harmful outcomes for ritual abuse and mind control victims in both the mental health and the legal arena. Harmful treatment decisions based on mis-diagnosis include lack of provision of treatment for trauma, incorrect and excessive use of medications, sometimes with severe and irreversible side effects, reinforcement of victims’ fears that they are hopelessly crazy and untreatable, long-term hospitalization, and involuntary hospital commitment. Harmful legal outcomes include incorrect findings of insanity, valid reports of abuse being viewed as delusional within law enforcement investigations and judicial proceedings, and forced conservatorship removing victims’ basic freedoms.
In order to judge the veracity of victims’ reports of these abuses, the clinician must have a basis for understanding what ritual abuse and trauma-based mind control programming are, that they do exist, the kinds of torture endured by victims of these abuses, and familiarity with the most common ritual symbols, artifacts, and holidays utilized by these abuser groups. A general overview of these now follows.
The Existence of Ritual Abuse
The term ritual abuse is often used broadly to include any organized abusive practice that furthers the abuser group’s ideology. However, the term is usually restricted to organized physical or sexual assault, often including homicide and severe psychological abuse, within the context of a spiritual practice or belief. Some definitions encompass any spiritual belief. But, most definitions use the term to refer to practices that involve physical and sexual abuse of children and adults, and human sacrifice, to propitiate and empower malevolent deities, such as Satan, but also including many polytheistic gods and goddesses.
A substantial body of psychological literature supports that ritualistic abuse is a real phenomenon that must be correctly assessed and treated (Belitz & Schacht, 1992; Bernet & Chang, 1997; Bloom, 1994; Boat, 1991; Boyd, 1991; Brown, 1994; Clark, 1994; Clay, 1996; Coleman, 1994a, 1994b; Comstock, 1991;, Comstock & Vickery, 1992; Cook, 1991; Coons, 1997; Cozolino, 1989, 1990; Crabtree, 1993; deMause, 1994; Driscoll & Wright, 1991; Edwards, 1991; Ehrensaft, 1992; Faller, 1994; Feldman, 1993; Fine, 1989; Finkelhor, Williams, & Burns, 1988; Fraser, 1990, 1991, 1993a, 1993b, 1997a, 1997b; Friesen, 1991, 1992, 1993; Golston, 1993; Gonzalez, Waterman, Kelly, McCord, & Oliveri, 1993; Goodman, Quas, Bottoms, Qin, Shaver, Orcutt, & Shapiro, 1997; Goodwin, 1993, 1994; Goodwin, Hill, & Attias, 1990; Gould, 1992, 1995; Gould & Cozolino, 1992; Gould & Graham-Costain, 1994; Gould & Neswald, 1992; Greaves, 1992; Groenendijk & van der Hart, 1995; Hammond, 1992; Harvey, 1993; Hill & Goodwin, 1989; Hornstein, 1991; Hudson, 1990, 1991; Ireland & Ireland, 1994; Johnson, 1994; Jones, 1991; Jonker & Jonker-Bakker, 1991, 1997; Katchen, 1992; Katchen & Sakheim, 1992; Kelley, 1989; King & Yorker, 1996; Kinscherff & Barnum,
1992; Kluft, 1988, 1989a, 1989b, 1994, 1995; Lawrence, Cozolino, & Foy, 1995; Leavitt, 1994, 2000a, 2000b; Leavitt & Labott, 1998a, 1998b, 2000; Lockwood, 1993; Lloyd, 1992; MacHovec, 1992; Mandell & Schiff, 1993; Mangen, 1992; Mayer, 1991; McCulley, 1994; McFadyen, Hanks, & James, 1993; McFarland & Lockerbie, 1994; Moriarty, 1991, 1992; Neswald & Gould, 1993; Neswald, Gould, & Graham-Costain, 1991; Noblitt, 1995; Noblitt & Perskin, 2000; Nurcombe & Unutzer, 1991; Oksana, 1994, 2001; Paley, 1992; Pulling & Cawthorn,1989; Raschke, 1990; Rockwell, 1994, 1995; Rose, 1996; Ross, 1995; Ryder, 1992, 1997; Ryder & Noland, 1992; Sachs, 1990; Sakheim, 1996; Sakheim & Devine, 1992; Scott, 2001; Sinason, 1994; Smith, C. 1998; Smith, M. 1993; Smith, M.R., 1992; Smith & Pazder, 1981; Snow & Sorenson, 1990; Stafford, 1993; Steele, H., 2003; Steele, K, 1989; Stratford, 1993; Summit, 1994; Tamarkin, 1994a, 1994b; Tate, 1991; Uherek, 1991; Valente, 1992, 2000; Van Benschoten, 1990; van der Hart, 1993; Vesper, 1991; Waterman, Kelly, Olivieri, McCord, 1993; Weir & Wheatcroft, 1995; Wong & McKeen, 1990; Woodsum, 1998; Young, 1992, 1993; Young, Sachs, Braun, & Watkins, 1991; Young & Young, 1997; Youngson, 1993.
The publishing arm of the American Psychiatric Association, the American Psychiatric Press, published a text in 1997 explaining the importance of correct assessment and treatment of victims of ritualistic abuse (The Dilemma of Ritual Abuse: Cautions and Guides for Therapists, edited by Fraser). One national survey of 2709 clinical psychologists found that 30% claimed to have seen at least one case of "ritualistic or religion-based abuse" and 93% of these psychologists believed the harm actually occurred (Goodman, Qin, Bottoms, & Shaver, 1994).
A review of the empirical evidence of ritual abuse is included in a book by Noblitt and Perskin (Cult and Ritual Abuse, 2000, Chapter 6). Noblitt and Perskin (2000) propose that “Cult and Ritual Trauma Disorder” be added as a new diagnosis to the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM). Inclusion of this diagnosis in the upcoming DSM would facilitate proper diagnosis and treatment of individuals with Ritual abuse/mind control traumatic stress, and would reduce mis-diagnosis of these individuals as having Schizophrenia and other psychotic or delusional disorders.
Trauma-Based Mind Control Programming
Organizations with a wide range of political and criminal agendas have historically relied on coercive interrogation and brainwashing of various types to force submission and information from enemies and victims, and to indoctrinate and increase cooperation in members and captives. In modern times, these techniques are used by political/military/espionage organizations, race/ethnic hate-groups, criminal groups (e.g., child pornographers and sex rings, and international traffickers of women, children, guns, and drugs) and exploitative and destructive cults with spiritual or other agendas. Methods of “thought reform” used by such groups include intimidation, social isolation, religious indoctrination, threats against victims or their loved ones, torture, torture of co-captives, and brainwashing through social influence or deprivation of basic needs, such as sleep or food (see Releasing the Bonds: Empowering People to Think for Themselves (2000), by Steven Hassan).
Trauma-based mind control programming is a term generally used for thought reform that goes beyond the above-described overt torture, intimidation, and brainwashing of the conscious mind, to covert installation of information in the unconscious mind through sophisticated, often technological, Machiavellian means. Mental health and law enforcement professionals working with severe trauma are increasingly seeing victims of such torture (Boyd, 1991; Coleman, 1994b; Hersha, Hersha, Griffis, & Schwarz, 2001; Katchen & Sakheim, 1992; Keith, 1998; Marks, 1979; Neswald & Gould, 1993; Neswald et al., 1991; Noblitt & Perskin, 2000; Oksana, 2001; Ross, 2000; Rutz, 2001; Ryder, 1992; Sheflin & Opton, 1978; Smith, 1993; Weinstein, 1990), and evidence has begun to surface in the legal arena (e.g., Orlikow v. U.S., 682 F.S. 77 (D.D.C. 1988).
Trauma-based mind control programming can be defined as systematic torture that blocks the victim’s capacity for conscious processing (through pain, terror, drugs, illusion, sensory deprivation, sensory over-stimulation, oxygen deprivation, cold, heat, spinning, brain stimulation, and often, near-death), and then employs suggestion and/or classical and operant conditioning (consistent with well-established behavioral modification principles) to implant thoughts, directives, and perceptions in the unconscious mind, often in newly-formed trauma-induced dissociated identities, that force the victim to do, feel, think, or perceive things for the purposes of the programmer. The objective is for the victim to follow directives with no conscious awareness, including execution of acts in clear violation of the victim’s volition, moral principles, and spiritual convictions.
One common function of trauma-based mind control programming is to cause the victim to physically and psychologically re-experience the torture used to install the programming should the victim consider violating its directives. The most common programs are unidimensional directives communicated during torture and impaired states of consciousness to, "Remember to forget" the abuse, and "Don't tell" about the abuse. Similar to this are pronouncements; claims, curses, covenants, etc., paired with abuse, that convince personalities they are controlled by evil entities, or forever malevolently defined as evil, physically or mentally ill, socially devalued and isolated, sexually enslaved, a murderer, a willing cult member, a coven member, etc.
Much trauma-based mind control programming is significantly more complex, more technological in its methods of installation, and utilizes the individual’s dissociated identities (personalities) to effect greater layering of psychological effects. Personalities are usually programmed to take executive control of the body in response to particular cues (hand signals, tones, etc.), and then follow directives, with complete amnesia for these events. Personalities are programmed to become flooded with anxiety or feel acutely suicidal if they defy program directives. Personalities are often programmed to believe that explosives have been surgically implanted in their bodies and that these will detonate if the individual violates orders or begins to recall the programming, the torture used to install it, or the identities of the programmers.
In highly sophisticated mind control, the individual is programmed to perceive inanimate structures in the unconscious inner landscape. “Structures” are mental representations of objects, e.g., buildings, grids, devices of torture, and other containers, that “hold” programmed commands, messages, information, and personalities. In many cases, walls are also installed that serve as barriers to hide deeper levels of programming and structures. Dissociated personalities perceive themselves as trapped within, or attached to, these structures, both visually (in internal imagery), and somatically (in experiences of pain, suffocation, electroshock, etc.).
Structures are mentally installed in early childhood, generally between two and five years of age. Torture, drugs, and even near death, are used in a variety of ways that make it extremely difficult for the child to mentally resist any of the programmer's input, and to ensure that memories of programing sessions remain dissociated. The child may be tortured on a device, and the personalities formed in this process then perceive themselves trapped on these devices. Or an image of an object may be projected on the child’s body or on a screen, or in virtual reality goggles, or a physical model of the object is shown. The programmer then tells the child that this object is now within him or her. Because the child is in an altered, disoriented state, and because the mind of the small child does not easily discriminate reality and fantasy (this process relies on the pre-school child’s use of magical thinking), the child now perceives the object as a structure within. Then, a code is installed, for the programmer to gain future access to the structure, to erase it, or to input new information.
Immediately after the structure is installed, the programmer will generally command traumatized personalities go to places in the structures, e.g., “Go inside the grid”. The programmer will generally also mentally install the perception of wires, bombs, and re-set buttons, to prevent removal of the structure. The child is usually shown something to make him or her perceive these as real, e.g., a button on the belly-button.
Kinds of Torture Endured in Ritual Abuse and Trauma-Based Mind Control
Knowledge of the methods of torture used within ritual abuse and trauma-based mind control provides a basis for recognition of related trauma disorders. Individuals subjected to these forms of torture may experience intense fear, phobic reactions, or physiological symptoms in response to associated stimuli. In some cases, the individual, or particular dissociated identities, experience a preoccupation with, or attraction to, related stimuli.
Victims may be able to describe the torture they have endured, or they may fear doing so. In many cases of ritual abuse and mind control trauma, the abuse remains dissociated when the individual first seeks treatment. Typically, the initial presenting problems are symptoms of anxiety, depression, or trauma derived from childhood sexual abuse, usually by a family member, who is eventually understood as a participant in the abuser group.
The following is a partial list of these forms of torture:
1. Sexual abuse and torture.2. Confinement in boxes, cages, coffins, etc., or burial (often with an opening or air-tube for oxygen).3. Restraint; with ropes, chains, cuffs, etc.4. Near-drowning.5. Extremes of heat and cold, including submersion in ice water, burning chemicals, and being held over fire. 6. Skinning for sacrifice or for torture. Pain-inducing drugs, chemicals, and/or adhesive tape can create an illusion of being skinned without permanent injury or scars.7. Spinning.8. Blinding or flashing light.9. Electric shock.10. Forced ingestion of offensive body fluids and matter, such as blood, urine, feces, flesh, etc.11. Being hung upside down or in painful positions.12. Hunger and thirst.13. Sleep deprivation.14 Compression with weights and devices.15. Sensory deprivation.16. Changes in atmospheric pressure (for example, using rapid pressure changes in a hyperbaric chamber to produce the "bends" and intense ear pain).17. Drugs to create illusion, confusion, and amnesia, often given by injection or intravenously.18. Oral or intravenous delivery of toxic chemicals to create pain or illness, including chemotherapy agents. 19. Limbs pulled or dislocated.20. Application of snakes, spiders, maggots, rats, and other animals to induce fear and disgust.21. Near-death experiences; such as by drowning or suffocation with immediate resuscitation.22. Forced to perform or witness abuse, torture and sacrifice of people and animals, usually with knives.23. Forced participation in child pornography and prostitution.24. Raped to become pregnant; the fetus is then aborted for ritual use, or the baby is taken for sacrifice or enslavement.25. Spiritual abuse to cause victims to feel possessed, harassed, and controlled internally by spirits or demons. 26. Desecration of Judeo-Christian beliefs and forms of worship; e.g., dedication to Satan or other deities.27. Abuse and illusion to convince victims that God is evil, such as convincing a child that God has raped her. 28. Surgery to torture, experiment, or cause the perception of physical or spiritual bombs or “implants”.29. Harm or threats of harm to family, friends, loved ones, pets, and other victims, to force compliance.30. Use of illusion and virtual reality to confuse and create non-credible disclosure.
To illustrate, ritual abuse survivors may experience intense phobic reactions to spiders or maggots (item 20). They may fear water and baths (items 4 and 5). They often fear hypodermic needles (item 18). They become easily too cold, too hot (item 5), or thirsty (item 12). They may have aversive reactions to cameras (item 23). They may become upset upon seeing babies, dolls, or particular animals, or they may strongly identify with abused and abandoned animals and children (items 22, 24, and 29). Sexual aversions are common (items 1, 23, and 24), as is vulnerability to repeated sexual victimization. Sexual compulsions and paraphilias, such as sadism, can also occur (Young et al., 1991).
Food aversions and eating disorders are common. Ritual abuse survivors may not be able to eat food that is brown or red because these remind them of feces and blood. They are often repulsed by meat, are vegetarian, or fast excessively, or regurgitate food, derived from forced ingestion of body matter and fluids (item 10).
Ritual abuse survivors, by and large, believe in the presence and power of spiritually evil forces, and often feel personally plagued by these (items 25, 26, 27, and 28). They may experience anxiety or an aversion to God and religion (items 26 and 27), or may alternatively be devout in their spiritual beliefs and practices.
Art productions, creative writing, and sandtrays, will often reflect their torture; including knives, religious symbols, frightening figures, coffins, burials, etc. Children unconsciously reenact elements of torture they have witnessed or experienced with toys and other objects. For example, a three-year-old boy wrapped a rope three times around his neck and pulled upward, as if to hang himself. A three-year-old girl sang about marrying Satan.
External or internal reminders of torture-related stimuli often precipitate dissociative responses, such as entering a trance state, falling asleep, or an other personality taking executive control of the individual. Torture-associated stimuli may also elicit disturbing impulses to re-enact unprocessed trauma, such as impulses to self-mutilate, or stab or sexually assault an other person.
Somatoform and conversion reactions occur frequently in response to ritual abuse and mind control trauma-reminders. Individuals often experience localized pain, especially genitourinary, musculoskeletal, and gastrointestinal, motor inhibitions, nausea, or even swelling in the affected area, prior to retrieval of any visual or narrative memory of the related torture. These are generally very distressing to the affected individual. Once the trauma is re-associated and processed within the context of psychotherapy or other forms of support, these somatoform and conversion reactions usually dissipate.
Survivors of trauma-based mind control often respond with distress to fluorescent lighting, since so much programming utilizes intense lighting (item 8). They may startle in response to a telephone ringing, related to programming to receive or make calls to abusers. They may believe they have microphones inside their heads that will relay their disclosures to their abusers (item 28). Fears of electronic or spiritual surveillance, and threats to loved ones (item 29), inhibit their ability to defy and escape their abusers or to disclose their abuse.
Victims of trauma-based mind control also usually experience intense or odd reactions to benign stimuli that were used in their programming. For example, they may have been programmed to “remember to forget” every time they see an apple, or to remember they are being watched every time they hear a police or fire siren. Similarly, they may make repetitive, robotic statements that do not make sense in the context of dialogue, e.g., "I want to go home", a common programmed statement intended to keep victims obedient to abuser groups and reporting to their abusers. Specific songs may be compulsively sung for similar programmed purposes.
All of these symptoms can occur prior to the individual having any conscious knowledge of the related abuse. This point is critical. Dissociative and neurobiological responses to overwhelming trauma (van der Kolk, McFarlane, & Weisaeth, 1996) often prevent these experiences from being processed into a coherent narrative memory. The diagnostician cannot rely on the patient to “put the pieces together” of their clinical picture.
Finally, generalized guilt and survivor guilt are strongly associated with ritual abuse, since participation in victimization of others is a mainstay of ritual abuse and mind control torture (items 22 and 29).
For more on recognition of symptoms specific to ritual abuse trauma, see Boyd 1991; Coleman 1994a; Gould 1992; Hudson 1991; Mangen 1992; Oksana 2001; Pulling and Cawthorn, 1989; Ross 1995; Ryder 1992; Young 1992; and Young and Young 1997.
Ritual Symbols, Artifacts, and Holidays Utilized by Groups Practicing Ritual Abuse
Practitioners of ritual abuse observe holidays and employ symbols and artifacts particular to their spiritual practices and beliefs. Victims may describe these, draw them, or be preoccupied with them. Commonly, victims experience increased distress as these dates approach and in relation to these symbols and artifacts. Recognition of ritual symbols, artifacts, and holidays alert the clinician to possible victimization in affected individuals.
Ritual holidays vary between groups, but some of the most common of these include victims’ birthdays, many Christian holidays (often in opposition to Christian doctrine and practice), All Hallows Eve through Samhain (October 29 through November 4), Candlemas (February 2), Beltane (May 1, and 10 days prior in preparation), Lammas (August 2), the vernal and autumnal equinoxes (March 21 and September 21), the summer and winter solstices (June 21 and December 21), full moons, new moons, and “Marriage to the Beast” in some practitioners of Satanism (September 5 to 7). Extreme distress, increased self-mutilation, suicidality, and hospitalizations in relation to ritual holidays are a strong indicator of ritual trauma (Ross, 1995).
Symbols and artifacts also vary, but commonly-reported ones include the five-pointed star within a circle (inverted in Satanism, upright in abusive witchcraft), the six-pointed star, the inverted Christian cross, the symmetrical cross in a circle, the letter “A” within a circle (the cross of the “A” extends beyond the circle), the Swastika within a circle (also utilized by Nazi-agenda groups), the circle, the triangle (upright or inverted), the Ankh, the infinity sign, lightening bolts, the Nero cross (peace symbol), the “all-seeing eye” in a triangle atop a pyramid (as on the United States dollar bill), altars upon which people are physically or sexually abused or sacrificed, black candles (often associated with sacrifice), white candles, other-colored candles, chalices, robes (often black, sometimes white and other colors), masks, swords and knives, snakes, spiders, the head of the goat, red (blood), black (death), brown (feces), and fixation on particular numbers (often, 6, 7, 8, 9, or 13).
The above-described holidays, symbols, and ritual artifacts, are generally not associated with victimization by political/military/espionage, race/ethnic hatred, or criminal groups (except the Swastika), unless they have a concurrent spiritual agenda. More detailed information on common ritual symbols, artifacts, and holidays utilized by groups with malevolent spiritual agendas are available in published accounts (See Boyd, 1991; Coleman, 1994b; Edwards, 1991; Katchen & Sakheim,1992; Pulling & Cawthon, 1989 (good illustrations); Ross, 1995; Ryder, 1992 (good illustrations); Oksana, 2001).
Primary Psychiatric Diagnoses for Individuals with Ritual Abuse and/or Mind Control Trauma
Using present diagnostic criteria, individuals with ritual abuse and/or mind control trauma generally hold a primary diagnosis of Post-traumatic Stress Disorder (PTSD), Disorders of Extreme Stress-Not Otherwise Specified (DESNOS), or a Dissociative Disorder, most commonly Dissociative Identity Disorder (DID). Secondary diagnoses often include other Anxiety Disorders (especially Panic Disorder and Phobias),
Mood Disorders, Eating Disorders, Sleep Disorders, Personality Disorders, Substance Abuse Disorders, Sexual Dysfunctions, Somatoform Disorders, Pain Disorders, Conversion Disorders, and stress-related physical diseases. The first step in accurate differential diagnosis from Schizophrenia is good working knowledge of the three primary diagnoses.
The reader is already likely familiar with the diagnostic criteria for PTSD. Briefly, these include three clusters of symptoms in response to having been exposed to a traumatic event. The first is persistent re- experiencing of the trauma in intrusive distressing recollections, recurrent distressing dreams, and the experience of the trauma re-occurring, as in re-living the experience, illusions, hallucinations, and dissociative flashback episodes, and intense psychological distress or physiological reactivity at exposure to internal or external cues associated with the trauma. The second is persistent avoidance of stimuli associated with the trauma, including the inability to recall an important aspect of the trauma, numbing of general responsiveness, and restricted range of affect. The third is persistent symptoms of increased arousal, including difficulty falling or staying asleep, irritability or outbursts of anger, difficulty concentrating, hypervigilance, and an exaggerated startle response.
Disorders of Extreme Stress-Not Otherwise Specified (DESNOS) are a relatively more recent diagnostic formulation not included in the DSM-IV (American Psychiatric Association, 1994), which perhaps better-capture the symptom picture of ritual abuse and/or mind control trauma survivors. These disorders are explained in depth on the world-wide-web in two scholarly articles (Luxenberg, T., Spinazzola, J., &. van der Kolk, B. (2001), Complex Trauma and Disorders of Extreme Stress (DESNOS) Diagnosis, Part One: Assessment, Directions in Psychiatry (21); Luxenberg, T., Spinazzola, J., Hidalgo, J., Hunt, C., &. van der Kolk, B. (2001), Complex Trauma and Disorders of Extreme Stress (DESNOS) Diagnosis, Part Two: Treatment, Directions in Psychiatry (21), see http://www.traumacenter.org/DESNOS.pdf)
The diagnostic criteria for DESNOS include six categories, as follows: 1) Alteration in regulation of affect and impulses, 2) Alterations in attention or consciousness (dissociative symptoms), 3) Alterations in self- perception (negative, trauma-related self-representations), 4) Alterations in relations with others (inability to trust, revictimization, or victimizing others), 5) Somatization, and 6) Alterations in systems of meaning (despair and hopelessness or loss of previously sustaining beliefs).
Dissociative disorders bear a bit more explanation, since these are generally the least recognized and understood, and because they are so strongly associated with Ritual abuse/mind control traumatic stress.
The DSM-IV Defensive Functioning Scale defines dissociation as follows; "The individual deals with emotional conflict or internal or external stressors with a breakdown in the usually integrated functions of consciousness, memory, perception of self or the environment, or sensory/motor behavior" (American Psychiatric Association, 1994, p. 755). Dissociation has become understood as a common response to trauma. Dissociative responses are generally believed to first arise during traumatic experiences and to be fortified by intrusive and chronic re-experiencing of these experiences. Common dissociative responses include self- induced trance states, numbing of psychological pain, bodily self-anesthesia, partial or full amnesia for abuse, depersonalization (feeling detached from oneself, as if in a dream), out-of-body experiences (the experience of observing one's self from without), and derealization (experiencing others or the world as less than real) (Briere, 1992; Ellenson, 1986, Hartman & Burgess, 1993; van der Kolk et al., 1996).
Dissociative responses also include many somatoform symptoms (Ross, 1997), such as transient or enduring numbness, insensitivity to pain, psychogenic stiffness or paralysis, genitourinary pain, gastrointestinal pain, musculoskeletal pain, pain on skin surfaces, disturbed smell or taste, psychogenic non-epileptic seizures, and impaired ability to see, hear, or speak. A body of research by Nijenhuis (2000) and colleagues argues convincingly that conversion and some somatization disorders are so intrinsic to dissociative disorders that they should be re-classified in the DSM as such. Nijenhuis (2000) has developed a scale to measure these, the Somatoform Dissociation Questionnaire (SDQ-20). An excellent book on the effects of trauma on health, injury, and disease is Robert Scaer’s The Body Bears the Burden: Trauma, Dissociation, and Disease (2001).
Attention to somatoform dissociative symptoms holds particular importance for assessment of Ritual abuse/mind control traumatic stress. Somatoform dissociative symptoms have been found to be associated with severity of reported childhood trauma involving physical contact or injury (Waller, Hamilton, Elliott, Lewendon, Stopa, Waters, Kennedy, Lee, Pearson, Kennerley, Hargreaves, Bashford & Chalkley, 2000). Since victims of ritual abuse and mind control have experienced extreme pain and torture, this may explain the great frequency of somatoform symptoms in this population (Oksana, 2001; Ryder, 1992). A study utilizing the SDQ-20 significantly differentiated Schizophrenia and Dissociative Disorders (Sar, Kundakci, Kiziltan, Bakim, & Bozkurt, 2000). Patients with dissociative disorders scored about twice that of patients with Schizophrenia. Thus, severity of somatoform symptoms may help differentiate patients with Ritual abuse/mind control traumatic stress from patients who should be diagnosed with Schizophrenia.
The most severe form of dissociative disorder is Dissociative Identity Disorder (DID). The DSM-IV defines its essential feature as "the presence of two or more distinct identities or personality states that recurrently take control of behavior" (p. 484). Van der Kolk et al. (1996) describe such identities as "distinct ego states that contain the traumatic experience, consisting of complex identities with distinct cognitive, affective, and behavioral patterns" (p. 307). DID is associated with chronic, intense, and early abuse, often involving a combination of physical, sexual, and emotional abuse, and frequently including experiences of profound neglect, family violence, and a generally chaotic home environment (Chu, Frey, Ganzel, & Matthews, 1999; Draijer & Langeland, 1999; Ogawa, Sroufe, Weinfield, Carlson, & Egeland, 1997; Putnam, 1997; Pynoos, Steinberg, & Goenjian,1996; Ross, 1995; Van der Kolk et al., 1996). Research suggests that its prevalence in the general population is at least 1 % and closer to 5% in samples of psychiatric patients (Ross, 1997).
Symptoms of DID include: 1) rapid personality changes, e.g., timid to aggressive, regressed to mature, female to male, 2) references to oneself in the third person, 3) reports of voices, primarily inside the head, 4) marked changes in appearance, skills, preferences, knowledge, memory, and physical complaints, 5) significant loss of time, and, 6) in children, reports that an animal or evil entity made them behave aggressively/destructively. In young children, personalities are often in a process of formation rather than fixed, thus the proposed diagnoses of "Incipient" DID (Fagan & McMahon, 1984) and "Dissociative Disorder of Childhood" (Peterson, 1996).
In ritual abuse and mind control trauma, a few personalities generally form in response to severe, early abuse, often in infancy. Personalities continue to branch off of these in response to ongoing trauma. Not uncommonly, these individuals have hundreds of personalities, receiving the diagnosis of Complex DID.
Adult survivors and child victims of ritual abuse and mind control often withhold dissociative experiences unless the subject is directly explored by the clinician. Many dissociative symptoms may be difficult for individuals to describe because they involve "negative" rather than "positive" experiences, such as, 1) amnesia, 2) emotional numbing, and 3) loss of self-awareness, time, or physical sensation. In DID, the host personality (“The personality that has executive control of the body for the greatest percentage of the time during a given time period”, Braun, 1986) may not report the presence of other personalities because the host fears them, is ashamed of them, wishes to deny their presence, or is not conscious of their existence (though internal personalities are usually aware of the host). In many cases, the individual withholds this information from the diagnostician for fear of not being believed or of being labeled “crazy”, psychotic, or Schizophrenic, a very common diagnostic error (Bliss, 1980; Kluft, 1987; Ross, 1997). However, survivors are more likely to reveal dissociative symptoms and related traumatic experiences to clinicians who demonstrate an understanding of dissociation, are respectful, and do not invalidate their experiences.
Psychological Tests in the Assessment of Ritual Abuse and/or Mind Control Trauma
The purpose of this paper is to provide guidelines for differential diagnosis within the context of the diagnostic interview and ongoing therapy rather than psychological testing. Yet, the literature on psychological testing with victims of ritual abuse, and a substantial body of research on psychological testing of DID and other dissociative disorders, inform our clinical understanding in ways that generalize to the clinical interview. These are conceptually incorporated in our differential diagnosis chart below. In complex cases in which diagnosis remains uncertain, psychological testing is indicated and the findings summarized herein can inform that process.
A review of the literature yielded few scholarly works specific to psychological testing of adult victims of ritual abuse. The most notable are by Mangen (1992), Noblitt (1995), and Leavitt and Labott (1998a, 2000).
Noblitt (1995) found that patients reporting ritual abuse had significantly higher scores than other psychiatric patients on two Minnesota Multiphasic Personality Inventory (MMPI) scales designed to measure Posttraumatic Stress Disorder (PTSD). They had a mean of 86.3 on the PK scale, (PTSD by Keane: Keane, Malloy & Fairbank, 1984) and a mean of 85.8 on the PS scale, (PTSD by Schlenger: Schlenger & Kulka, 1989). Patients not reporting ritual abuse had a mean PK score of 58.3 and a mean PS score of 58.7. For patients reporting ritual abuse, 91% of them had scores in the clinically significant range (above 65) on at least one of these two scales. Both scales were developed based on research comparing MMPIs of Vietnam veterans with Posttraumatic Stress Disorder to other psychiatric patients.
Leavitt and Labott (2000) compared Rorschach results of three groups of patients; 1) patients reporting child sexual abuse within Satanic cults; 2) patients reporting child sexual abuse without ritual abuse; and 3) non-abused patients. The first two groups had histories of amnesia for their sexual trauma, memory recovery after the age of 18 years, and an absence of psychotic or neurologic symptoms. Groups were compared for frequency of 41 Rorschach content responses related to Satanic ritual abuse, selected by four experts in ritual trauma. The group of patients reporting abuse within Satanic cults gave significantly more Rorschach responses with Satanic content. The following specific percepts significantly differentiated the groups: robe, mask, body mutilated, babies damaged, ritual ceremony, threatening eyes, blood everywhere, special knife, goat reference, bondage, torture, sacrifice, hooded figure, altar, blood rituals, and circle. A second study revealed that these results were unrelated to patients’ degree of media and hospital milieu exposure to the subject of Satanic ritual abuse. In fact, less media exposure was associated with production of more Satanic content in patients reporting ritual abuse, evidence that reports of ritual abuse are not primarily the product of exposure contagion.
In an earlier study, Leavitt and Labott (1998a) found that patients reporting Satanic ritual abuse provided more Satanic-content responses in a word association test than patients reporting non-ritual sexual abuse. They also provided fewer normative responses, understandable given the pervasive nature of ritual trauma and the paucity of normal childhood experience for so many of these victims.
Mangen (1992) performed approximately 25 psychological evaluations with patients already identified as having been victimized within Satanic cults, including the Wechsler Adult Intelligence Scale-Revised (WAIS-R), Rorschach, Thematic Apperception Test (TAT) or other story-telling test, a human figure drawings, and more.
Mangen found that the “testing” situation itself often induced great fear in these patients, related to the frequent “tests” of abilities within ritual abuse. Test stimuli, even benign or familiar stimuli, often acted as trauma reminders and precipitated trauma reactions and dissociative “switching” of personalities. He observed that “many responses given by these patients sound blatantly psychotic” (p. 154), but closer scrutiny revealed that these were derived from the ritual abuse and the traumatized level of functioning. He explains the importance of understanding ritual abuse practices, symbols, holidays, etc., as emphasized above.
Mangen found these individuals were of at least average intelligence. However, signs of cognitive slippage and inefficiency occurred as trauma impinged on thought processes. Idiosyncratic, personalized, and even bizarre responses to test stimuli were common. E.g., intelligence tests involving numbers, and in particular, having to repeat series of numbers backwards, often disorganized patients’ responses, since numbers and reversal of numbers and letters are common in ritual practices and programming. Mangen noted that words often lost their meaning as symbols, and were perceived as dangerous in themselves, related to abusers communicating deadly messages with words, and punishment by abusers for incorrect verbal responses. Visual images also disorganized thought processes. E.g., one woman froze when given puzzle pieces of a human figure to assemble. When asked what had happened, she “switched” into a young personality who explained that she had participated in rituals involving people being cut into pieces, but had never been told to try to put the people back together.
Mangen emphasized that such disorganized episodes are frequent, but exist side-by-side with trauma- free spheres of cognitive functioning. He suggests that the traumatized thought processes are state-dependent, and that these patients readily enter states of traumatized functioning.
Mangen’s Rorschach observations are especially revealing. Patients tended to provide images that were perceptually accurate (good form); i.e., they were largely consistent with shapes in the inkblot. In contrast, patients with Schizophrenia often have poor perceptual accuracy (poor form) on the Rorschach, a sign of more impaired perceptual and thought processes.
Though form was generally adequate, associations to the blots were replete with traumatic imagery. E.g., a perception of a person might fit the blot, but the associations might include themes of cutting and murdering babies, eating flesh, evil, etc., additions that would appear bizarre if not for the ritual trauma. Such trauma-driven associations might be made with flat affect or flooded affect. In some cases, perceptual distortions (poor form) were more central, but even these were often resolved in light of the abuse. For example, one patient perceived a person with women’s breasts and a penis, an incongruous combination (INCOM) that might indicate psychosis, if not for the fact that some sexual rituals involve people costumed to appear bi-gender. Yellow was perceived by an other patient as angry and as urine “poured all over me”. This response becomes understandable if the clinician knows that abusers often urinate on the victim, in some cases with the intent to dominate the spirit of the victim with their own spirits.
Mangen explains that drawings also contain elements that would appear bizarre without an understanding of the underlying trauma. For example, trees may contain eyes, hidden people, and blood dripping from severed limbs. Moore (1994) notes that in human figure drawings of ritual abuse victims, arms often abruptly end, appear torn off or jagged, or have unusual endings unlike hands. Ritual acts, symbols, candles, pentagrams, inverted crosses, robes, dripping blood, etc., may be graphically represented, particularly if the abuse is conscious. Cohen and Cox (1995) include a series of drawings depicting the unfolding of memories of an adult woman ritually abused as a child, replete with graphic memories of abusive rituals, ritual artifacts, her terror, phallic symbols of sexual abuse, and dissociative responses, such as multiple self- representations in one drawing, and changes in developmental level across drawings in relation to the age of the personality making the picture.
Mangen reports that ritual abuse victims demonstrate a damaged experience of self on projective tests, such as the Rorschach and TAT. Responses demonstrate a lack of self-agency, that is, a sense of lack of control over one’s life and actions. Figures are often perceived as helpless or passive. Body integrity is often impaired; figures are seen as broken, devoured, harmed, etc. Self affect is inconsistent and incongruent. For example, a figure may be described as frightened and laughing, evil and good, etc. Dissociative processes are evident in illogical shifts and transpositions. TAT stories include confusion in regard to time, states of waking and sleeping, life and death, here and not here, and sudden changes in what characters know, think, and want.
TAT stories reflect interpersonal estrangement and malevolence. Themes of caring and kindness tend to be fleeting. Themes of deception and betrayal are common; “things are not what they seem”. Kind adults turn threatening. Child figures may feign compliance, but are described as actually pretending or escaping in their minds (dissociating). Responses are consistent with the devastating and pervasive abuse these victims have experienced, so often including immediate family members.
Affect dysregulation and emotional intensity pervade test responses. Primitive violent imagery related to ritual trauma is common in Rorschach responses and TAT stories. There is a paucity of positively tinged affective experiences, such as love and hope. Terror and despair dominate. Fear of annihilation and abandonment are more common than fear of loss of love. Some responses may reflect identification with aggressors.
Dissociative responses are observed throughout the evaluation process. Blocking of affect may occur as trauma is described. Overwhelming stimuli can precipitate switching of personalities. There may be obvious changes in vocal presentation and general demeanor. Personalities may identify themselves by name. They may relay accounts of horrible abuse unknown to the host and the host may return with complete amnesia for the event. Or dissociative episodes may be more subtle, and not distinguished unless the evaluator looks for amnestic gaps, such as the repetition of test questions later in the evaluation process to determine if prior responses are recalled.
Mangen explains that the patient may not be able to reveal the “secret” of the abuse and that personalities who identify with the cult experience tend not to present themselves. Thus the clinician must work with the patient to “help make the invisible visible” (p. 155). However, he states that much more research is needed on the use of psychological testing in identifying severe trauma, dissociation, and in particular ritual trauma, to help clinicians to recognize patients who are still preserving the “secret” and not yet revealing their ritual abuse.
Since 1989, a number of assessment and screening tools have been proven very useful in discovering dissociative symptomatology. These tools can play a critical role in differentiating Dissociative Disorders from Schizophrenia (Steinberg, Cicchetti, Buchanan, Rakfeldt & Rounsaville, 1994; Welburn, Fraser, Jordan, Cameron, Webb, & Raine, 2003), thereby making an important contribution to differential diagnosis of Ritual abuse/mind control traumatic stress from Schizophrenia. Administration and scoring do not require specialized training in psychological testing. The structured interviews (DDIS, SCID-D-R, SIDES) require knowledge of dissociation. A helpful description of most of these tools is included in the International Society for the Study of Dissociation 2005 Guidelines for Treating Dissociative Identity Disorder in Adults, available online at http://www.issd.org/indexpage/treatguide1.htm#diagnosticinterviewing. These measures include:
The Dissociative Experiences Scale (DES), a 28-item self-report measure (Carlson & Putnam, 1993; Carlson, Putnam, Ross, Torem, Coons, Dill, Loewenstein, & Braun, 1993).
The Dissociation Questionnaire (DIS-Q) (Vanderlinden, Van Dyck, Vandereycken, Vertommen, & Verkes, 1993).
Questionnaire of Experiences of Dissociation (QED) (Riley, 1988).
The Multidimensional Inventory of Dissociation (MID) (Dell, 2004). The Multiscale Dissociation Inventory (MDI) (Briere, 2002)
The Clinician Administered Dissociative States Scale (CADSS) ( Bremner, J.D., Krystal, J.H., Putnam, F.W., Southwick, S.M., Marmar, C., Charney, D. S., & Mazure, C.M. (1998). Measurement of dissociative states with the clinician-administered dissociative states scale (CADSS). Journal of Traumatic Stress, 11, 125-136)
The Dissociative Disorders Interview Schedule- DSM-IV Version (DDIS), a highly structured interview administered in 30 to 45 minutes (Ross, 1989; Ross, 1997).
Structured Clinical Interview for DSM-IV Dissociative Disorders-Revised (SCID-D-R) (Steinberg, 1996), a highly structured interview administered in 45 to 180 minutes.
Structured Interview of Disorders of Extreme Stress (SIDES) (Pelcovitz, van der Kolk, Roth, Mandel, Kaplan, & Resicket, 1997). (This tool for assessing extreme traumatic stress includes a subscale, “Alterations in Attention or Consciousness”, which has sub-categories of amnesia, dissociative episodes, depersonalization)
Somatoform Dissociation Questionnaire (SDQ-20), (Nijenhuis, 2000).Adolescent Dissociative Experiences Scale-II (A-DES) (Armstrong, Putnam, Carlson, Libero, & Smith, 1997).
Differential diagnosis of children with ritual trauma is beyond the scope of this paper. However, three widely-used scales that screen for dissociative disorders are included for reference:
Children's Perceptual Alteration Scale (Evers-Szostak & Sanders 1992). Child Dissociative Checklist (Putnam, Helmers, & Trickett,1993;Version 3). Child Dissociation Problem Checklist (Peterson, 1991).
A substantial body of research has identified a number of Rorschach indicators that differentiate DID and other dissociative disorders from other mental disorders (Armstrong, 1991; Danesino, Daniels, & McLaughlin, 1979; Labott, Leavitt, Braun, & Sachs, 1992; Labott & Wallach, 2002; Leavitt & Labott, 1998b; Lovitt & Lefkoff, 1985; Scroppo, Drob, Weinberger, & Eagle, 1998; Silberg, 1998; Wagner, Allison & Wagner, 1983; Wagner & Heise, 1974; Young, Wagner, & Finn, 1994).
Not surprisingly, individuals with DID produce more traumatized content than many other populations, including perceptions of blood, anatomy, and morbidity (images of things that are damaged, diseased, mutilated, dead, etc.), and assault or pursuit, consistent with their history of severe trauma and intense somatic concerns. Traumatic imagery in the blots can precipitate intense anxiety, flashbacks, autohypnotic trance states, or a change in personality. Silberg (1998) found that dissociative children and adolescents perceived in a battery of tests (including the Rorschach) more images of torture, mutilation, and malevolent religiosity (sacrificial ceremonies, devils, etc.) than other patients. Some reported that symbols of Satan or devils had been used to terrorize them.
Patients with DID have an elevated number of responses depicting fragmentation, that is, the perception of objects as divided, torn, cut, broken, or split, paralleling their lack of integration of consciousness and a sense of damaged body integrity. They tend to form highly atypical images (high Xu and low X+% in the Exner (1978) system), indicating a tendency to see the world in an unconventional manner. They tend to see incompatible relationships in the blots, such as inappropriate condensation of images into single objects (INCOM) and implausible relationships between objects (FABCOM). These findings derive, in part, from dissociation and their heightened imaginative capacity, and can appear like Rorschach responses of Schizophrenia in their divergence from conventionality and reality.
However, patients with DID tend to see few severely distorted responses (X-) and more whole and real objects than part and imaginary objects, in contrast to patients with Schizophrenia. They also tend to have at least one human movement response with unusually well-articulated form (M+), an indicator of normal psychological development that is atypical of psychotic subjects. They also tended to have very large number of responses involving the perception of depth, distance, or dimensionality (high FD), which is associated with a good capacity for intellectual self-observation and introspection (Armstrong & Loewenstein, 1990). This also corresponds with derealization experiences in which things appear far away, distorted, or unreal.
DID patients have some tendency to respond to color more than form in color responses (total CF and C responses is greater than total FC responses), including color responses of both positive (e.g., a flower) and negative (e.g., blood) connotations (Wagner et al, 1983, 1994). Color dominating form is related to weak regulation of affect and behavior, also consistent with severe trauma and subsequent dysfunctionality.
DID patients have a large number of responses involving the perception of movement (e.g., a bird flying, a woman sewing). This is associated with heightened imaginative capacity and is consistent with the capacity of individuals with DID to dissociate (self-induced trance, retreat into their inner world, switching to other personalities) to mentally escape trauma. Dissociative children and adolescents have also been found to be fantasy-prone, relying more than other patients on dissociative coping mechanisms such as pretending, forgetting, wishing, sleeping, extreme dichotomization of things, and mental magical transformations (e.g., evil becomes good, dead become alive) (Rhue, Lynn, & Sandberg, 1995; Silberg, 1998).
These Rorschach indicators have relevance for diagnostic interviews with victims of ritual abuse and mind control since most of these victims are highly dissociative. The clinician should expect intrusive traumatic images and fears to impinge on thought processes and to generate dissociative responses. Identity and self- expression are likely to be incohesive. The environment may be perceived and described unconventionally. Moderate dysfunction in regulation of behavior and affect can be expected. These effects are likely to be magnified in ritual abuse and mind control trauma since the abuse is so extensive, and often begins in infancy or early childhood.
Sources of Mis-Diagnosis of Schizophrenia in Cases of Ritual Abuse/Mind Control Traumatic Stress
Symptoms of PTSD, DESNOS, and Dissociative Disorders often present as similar to symptoms of Schizophrenia. Hallucinations, delusions, and thought disorders, long believed to be the hallmark of Schizophrenia, are now being understood as commonplace to trauma disorders. Disorders of extreme stress have a profound effect on cognition, perception, identity, social relationships, stress-tolerance, and regulation of affect and behavior. And dissociative phenomena disturb the integrative functions of consciousness, memory, identity, and sensory perception severely enough that the clinical picture begins to resemble the confusion of Schizophrenia. Thus the high rates of this mis-diagnosis, and years of treatment before proper diagnosis (Bliss, 1980; Kluft, 1987; Ross, 1997).
Schneiderian first rank symptoms, historically considered to be classic features of Schizophrenia, are actually more prevalent in DID than in Schizophrenia. A comparison of 1739 schizophrenics with 368 MPD (Multiple Personality Disorder; the designation for DID in 1990) patients found that schizophrenics averaged 1.3 Schneiderian first rank symptoms, while MPD subjects averaged 4.9 (Ross, Miller, Reagor, Bjornson, Fraser, & Anderson, 1990).
Similarly, Ellason and Ross (1995) compared 108 patients with DID patients with 240 patients with Schizophrenia. They found that positive symptoms were more severe in the DID group, while the negative symptoms were more severe in Schizophrenia. Positive symptoms include delusions, conceptual disorganization, hallucinatory behavior, excitement, grandiosity, suspiciousness, and hostility. Negative symptoms include blunted affect, emotional withdrawal, poor rapport, passive-apathetic social withdrawal, difficulty in abstract thinking, poverty of thought and spontaneous activity, and stereotyped thinking/behavior.
Schneiderian positive symptoms common in DID include hallucinations of voices commenting on one's behavior, conversing, or arguing (voices are the most common symptom, Ross et al., 1990); thought insertion (the belief that thoughts have been placed into one's mind); thought withdrawal (the belief that thoughts are being taken from one’s mind); audible thoughts (hearing one's thoughts spoken aloud); delusions of control; and somatic passivity (the belief that the body is being influenced by an external force or power) (Kluft, 1987; Ross et al., 1990). True thought broadcasting (the belief that one’s thoughts are transmitted to others all around, often via some form of media), a Schneiderian first rank symptom, tends not to occur in DID. However, a suspicion that others are able to read one’s mind, especially a parent or a therapist, does occur in DID (Kluft, 1987).
When trauma-based disorders originate in experiences of ritual abuse and/or mind control, diagnostic questions become even more complex, and mis-diagnosis of Schizophrenia more likely.
Much of the basis for mis-diagnosis lies in the DSM-IV’s definitions of delusions and hallucinations, and the diagnostic criteria for Schizophrenia.
The DSM-IV defines a delusion as, “A false belief based on incorrect inference about external reality that is firmly sustained despite what almost everybody else believes and despite what constitutes incontrovertible and obvious proof or evidence to the contrary. The belief is not one ordinarily accepted by other members of the person's culture or subculture (e.g. it is not an article of religious faith)...” (American Psychiatric Association, 1994, p. 765).
Belief in the existence of ritual abuse and mind control is not in the realm of acceptance in mainstream Western culture, and therefore likely to be mistaken for delusional. Information on ritual abuse and mind control is generally unavailable due to: 1) the secrecy preserved by the underground abuser groups, 2) profound dissociative responses in the victims limiting their own knowledge of their abuse history, 3) victims’ fear of disclosure (Fraser; 1997b; Young & Young, 1997), 4) abusers’ use of sophisticated mind control techniques designed specifically to prevent victims from gaining any conscious awareness of the abuse, 5) use of torture and illusion to instill bizarre “cover memories” to undermine victims’ credibility and make them appear insane, and 6) claims that memories of ritual abuse are false, grossly exaggerated, or the product of bad therapy, by organizations that have had considerable influence in the media and much presence in the courts, such as the False Memory Syndrome Foundation (Brown, Scheflin, & Hammond, 1998; Coons, 1997; Whitfield, Silberg, & Fink, 2002; Young & Young, 1997).
This coordinated effort to discredit reports of ritual abuse and mind control is supported by the natural human tendency to dismiss these heinous crimes as impossible because they are too disturbing to believe. Health and law enforcement officials often believe victims’ accounts upon first hearing them. But within hours or days, many come to view the victim as psychotic. This is often based in a emotional aversion for the material, albeit often an unconscious reaction. In contrast, clinicians and law enforcement officials who accept that these crimes are real are often ostracized by their colleagues, and often experience significant secondary traumatic stress (Perlman, 1995), and painful shifts in their view of humanity, their communities, and the world.
The subject of ritual abuse also has little presence in recent mainstream professional literature. A good many psychology books and journal articles exposed ritual abuse in the early 1990s. But since 1995, the number of publications has dropped dramatically, as mental health professionals reeled from legal and media accusations of “implanting false memories” of child abuse, particularly ritual abuse. Since then, many psychotherapists treating victims of these abuses have become very guarded about divulging their clinical findings, and many medical and mental health professionals now peremptorily dismiss all reports of ritual abuse as delusional.
To the uninformed or misinformed clinician, common beliefs and behaviors associated with ritual trauma and mind control are indistinguishable from many types of delusions associated with Schizophrenia or Delusional Disorder, per DSM-IV definitions (pp. 765- 766). Reports of torture by organized abuser groups conspiring to silence their victims are easily mistaken for bizarre (implausible) and persecutory delusions. Reports of explosives within the body or surgical implants controlling oneself (common beliefs installed in technological mind control) can easily be confused with somatic delusions. Similarly misinterpreted are fear responses to benign stimuli, that were in actuality utilized in the victim’s trauma or programming. Programming can also cause compulsive behaviors that appear bizarre when viewed out of context, such as robotic, repetitive statements or singing songs at inappropriate times, unusual hand movements, patterned self-mutilation, etc. These behaviors and beliefs appear bizarre, possibly psychotic, if the history of ritual trauma and coercive mind control remain unrecognized.
These victims often report abuse by well-known individuals or government, military, espionage, religious, business, or entertainment institutions. They may allege that such people and institutions are involved in organized child pornography, pedophilia, trafficking of women and children, etc. Many clinicians reflexively view such reports as delusional rather than considering them further. In fact, quite a few facets of victimization by ritual abuse and mind control can generate such beliefs, as follows:
1. These beliefs are often derived from false claims by victims’ abusers and programmed illusions used to perpetuate these beliefs. It appears that most abuser groups seek to convince their victims that they are the most powerful and formidable group, the most well-connected to prominent individuals and organizations. Many groups call themselves “the Illuminati”, to distinguish themselves as the most enlightened and spiritually powerful. They claim to be direct descendants of the Knights Templar, the 16th Century Roshaniya of Afghanistan (Daraul, 1997), the Pharaohs of Europe, etc. All such claims are highly unlikely, but help control victims with fear.
2. For many victims of ritual abuse and mind control, the first indication of their trauma is a poorly- defined state of fear or a sense that something is not right. Dissociation and programming make any true memory consciously inaccessible. Naturally driven to determine the source of their uneasiness, they read books, search the internet, and make inquiries. They come upon information about ritual abuse and mind control and this information “resonates” with them. These individuals begin to piece together their lives “from the outside in”, since they cannot yet accomplish this “from the inside out”. This approach can result in victims believing they were abused by individuals or institutions unrelated to their abuse.
3. Such allegations can originate in the individual’s own personalities who seek to confuse, overwhelm, and terrify the host personality. A personality loyal to one abuser group may make false allegations against particular individuals or institutions that are viewed as rivals. Or, a personality may seek to keep the host in a state of generalized fear of everyone to prevent access to the memories of the actual abuse.
4. These perceptions may be based entirely or primarily in actual experience. For example, Senator John DeCamp’s book, The Franklin Cover-Up: Child Abuse, Satanism, and Murder in Nebraska, 1992, has carefully documented a case involving allegations of ritual abuse involving prominent community and political figures. The clinician should exercise caution to ensure that his or her cultural biases, spiritual beliefs, and political opinions do not bias diagnostic determinations when allegations are made against prominent figures or institutions.
Abusive mind control usually endeavors to make victims believe that their thoughts are always heard, via surgical implants or electronic surveillance. And victims of ritual trauma usually believe that spiritual entities attached in rituals are now controlling them, commanding them, or reading their thoughts. These can appear much like delusions of thought broadcasting, being controlled, and thought insertion. Yet, these are effects that most individuals would undergo if so-traumatized, rather than derived from a neurological disease process, a proven factor the development of Schizophrenia.
The DSM-IV defines hallucinations as, “A sensory perception that has the compelling sense of reality of a true perception but that occurs without external stimulation of the relevant sensory organ”, (p. 767) with or without insight that it is a hallucination. The term is not ordinarily applied to perceptions that occur while falling asleep or awakening. Illusions are distinguished from hallucinations; “an actual external stimulus is misperceived or misinterpreted” (p. 768).
This definition is very broad and does not address the multiple etiologies of hallucinations. When hallucinations are present, many diagnosticians consider Schizophrenia, severe mood disorders, and processes that directly effect the physiology of the brain, such as neurological lesions and diseases, medical illnesses that affect brain physiology, toxins, and substance abuse.
Hallucinations are still not widely attributed to trauma-based disorders and dissociative experiences. Yet, hallucinations are commonly associated with trauma, and are more likely to be present when the trauma is severe, of earlier onset, when it includes sexual abuse, and when violence extends into adulthood.
Read and Argyle (1999) found that psychiatric inpatients reporting a history of sexual or physical abuse had a high frequency of auditory hallucinations, particularly command hallucinations to kill oneself, and paranoid ideation. They write; “Half of the symptoms for which content was recorded appeared to be related to their abuse. An analysis of the relationships between types of abuse and specific symptoms suggested that hallucinations may be more common than delusions or thought disorder among patients who have been sexually abused, particularly among those who have experienced incest, and that delusions may be more related to having been physically abused” (p. 1467). Flashbacks of ritual trauma regularly involve auditory and visual hallucinations of abusers, and somatic sensations of torture being re-lived.
Greater perceptual distortions are likely to occur when child abuse is of earlier onset, longer duration, involves a number of perpetrators, and when abusers are more closely related to the victim (Sacco & Farber, 1999). Read, Agar, Argyle, and Aderhold (2003) found that 47% of community mental health center patients who were abused as children experienced hallucinations compared to 18% of patients with no abuse. Findings were significant for hearing voices, and command, visual, tactile, and olfactory hallucinations. Adult abuse alone did not generally predict hallucinations. However, patients with both child sexual abuse and adult sexual abuse were more likely to experience delusions and/or thought disorders. Mueser and Butler (1987) found that war veterans with PTSD who had auditory hallucinations had significantly more combat exposure than those without hallucinations. These findings hold great relevance for victims of ritual abuse and mind control, since the abuse often extends into adulthood, and may even be ongoing when the individual seeks treatment.
Bliss (1980) is his article distinguishing features of Schizophrenia and “hysterics with multiple personalities” (the diagnostic term for Dissociative Identity Disorder in 1980) observed the following about visual hallucinations in DID:
What is seen is usually life-like and real, and corresponds to the kind of visual hallucinations schizophrenics often report. These contrast with weird, bizarre, polychromatic visions seen by alcoholics in delirium tremens, or those found in other toxic deliria. (P. 1396)
While toxic deliria often produce visual hallucinations that remind one of Fantasia on LSD (more fantastic and distorted than the visual hallucinations seen with ritual trauma), it is important to note that victims tortured with electroshock, a common means of inducing pain in abusive mind control, often experience flashes of light (often white, blue, red, orange, and yellow) as components of their flashback experiences.
Many mental health professionals continue to mistake reports of voices of dissociated identities for auditory hallucinations. And some victims of ritual abuse have personalities perceived to be animals which, when in executive control, may behave as such; growling, crouching, etc. In some ritual trauma, victims are locked in cages, starved, kept in dark or cold environments, and encouraged to take on animal behaviors and identities. Hendrickson, McCarty, and Goodwin (1990) report that DID patients with animal alters report being forced to live like an animal, exposure to bestiality, and being forced to witness or participate in torture, mutilation, and killing of animals to terrorize, punish, and control them. This clinical phenomenon, which at first may seem like psychotic behavior, has a discernable basis in the patient’s trauma history.
If the functional host personality loses executive control of the mind and body, and less functional alters take over long-term control, dysfunctionality can be quite global. Personalities who serve to “hold” the most severe trauma apart from the host may be in constant terror and appear blatantly psychotic. Or completely non- emotional personalities may take executive control in efforts to contain affect flooding. These may be nonresponsive, appear catatonic, and may even deny their true identity, symptoms easily mistaken for psychotic.
The DSM-IV states that Schizophrenia is diagnosed “if delusions are bizarre or hallucinations consist of a voice keeping up a running commentary on the person’s behavior or thoughts, or two or more voices conversing with each other” (American Psychiatric Association, 1994, p. 285), with corresponding social or occupational dysfunction, for a duration of at least 6 months. Diagnostic exclusions are limited to Schizoaffective, Mood, Substance, and Pervasive Developmental Disorders. By these criteria, when “bizarre delusions” or the above-described voices occur, Schizophrenia should be diagnosed, even if these occur only during the active phase of Dissociative, Post-traumatic, and Acute Stress Disorders. Clearly, this is a troubling source of mis-diagnosis in cases of ritual trauma, and in disorders of dissociation and extreme stress in general.
Distinguishing symptoms of actual ritual abuse from true psychosis is further complicated by the fact that in some cases, the first can eventually develop into the second. Ritual trauma and mind control often cause victims to perceive abusers as omniscient, omnipresent, and capable of almost anything. Many victims isolate themselves socially, due to fear of people or feelings of unworthiness, and may not be able to work. Having little or nothing to ground them back to outer reality, they retreat further into inner nightmarish worlds and their fears can grow unchecked. In cases of organized criminal abuse, perpetrators may still be monitoring, or even abusing, the individual. Prolonged states of dread and hypervigilance eventually gain their own momentum and “outrun” actual events. In an attempt to attach meaning to this state of fear, victims may seek answers from unreliable sources. In particular, the internet is a valuable source of useful information on ritual abuse and mind control, but is also a source of much misinformation. The individual may finally develop an acute traumatic stress reactive psychosis, in which reality testing is severely compromised. The fear can escalate until it is generalized to almost everything and everyone in the environment, which can closely resemble the delusional state of acute paranoid Schizophrenia. In actuality, this clinical picture is more closely related to the stress-induced deterioration in dissociative patients that was in years past termed Hysterical Psychosis (Tutkun, Yargic, & Sar, 1996). Per the DSM-IV, Brief Psychotic Disorder would be the most fitting diagnosis, but this lacks the etiological specificity of Hysterical Psychosis. Prolonged extreme stress can eventually result in generalized and extended gross dysfunction, including catatonic states. The DSM-IV provides no diagnostic category that fits this most chronic and deteriorated presentation.
In some cases, trauma may contribute to the pathogenesis of Schizophrenia. Read, Perry, Moskowitz, and Connolly (2001) propose a traumagenic neurodevelopmental model of Schizophrenia. Read et al. (2003) suggest that the heightened sensitivity to stress which is found in Schizophrenia is, for some patients, related to neurodevelopmental changes caused by childhood trauma. They cite numerous studies showing a high prevalence of childhood abuse and trauma in psychiatric inpatients diagnosed with severe mental disorders. They also point out many similarities between the effects of early trauma on the developing brain and neurobiological abnormalities associated with Schizophrenia. These include “overreactivity of the hypothalamic-pituitary-adrenal (HPA) axis; dopamine, norepinephrine, and serotonin abnormalities; and structural changes to the brain such as hippocampal damage, cerebral atrophy, ventricular enlargement, and reversed cerebral asymmetry" (p. 319). These neurobiological similarities should be interpreted cautiously, but are certainly consistent with the significant overlap in clinical symptoms of severe trauma disorders and Schizophrenia.
In some cases, an individual will have both Schizophrenia and Ritual abuse/mind control traumatic stress (these individuals are seen most often in inpatient settings). Fortunately, in most cases, these disorders are distinct, and readily differentiated by clinicians experienced with both populations.
Some victims of ritual abuse and mind control appear to have suffered abuse extensive enough to result in irreversible brain damage (e.g., prolonged oxygen deprivation or extensive electroshock). In such cases, the individual can appear much like a individual with chronic Schizophrenia or organic psychosis.
Spiritual Factors
Most ritual abuse victims believe in the existence of God, a rival force of evil, such as Satan, and lesser evil entities, such as demons. Many report having a personal relationship with God, Jesus, angels, etc., as a source of divine guidance and support, often beginning with a profound spiritual experience while being tortured as a child. They may describe a close spiritual connection to other children abused with them in rituals, and may even believe they hold parts of the spirits of sacrificed children within themselves, to help these spirits. They may believe that God has directed them to help other victims of ritual abuse or to expose these crimes, and may be helping others through support networks, writing a book, etc. They are often deeply committed to their faith. Many worship within mainstream religions, and others only within individual spiritual practice. Other survivors have anxious and aversive reactions to organized religion, particularly Judeo-Christian religions, as a direct result of rituals involving desecration of Judeo-Christian houses of worship and religious symbols (e.g., the cross), and torture and programming to prevent faith in the Judeo-Christian God.
Ritual abuse victims also commonly experience the presence of evil spiritual entities, both internally and externally. They may believe they have malevolent spiritual attachments within themselves, and may feel plagued or controlled by spirits of living, or even dead, abusers. Some victims believe that they have been possessed by evil spirits or demons, briefly or long-term. These phenomena are often restricted to only particular personalities.
Some survivors believe they have spiritual or supernatural powers and that they are engaged in a battle of good against evil. Many engage in spiritual warfare, or even exorcism of demons, usually within Christian faiths, to protect themselves from forces of extreme evil associated with their childhood ritual abuse, and which they believe still intend them harm. Some practice “white magic” or “Wicca” in efforts to empower themselves.
Many victims of ritual abuse report being telepathic or clairvoyant, and may be superstitious and rely on magical thinking. These characteristics are shared by many patients with DID who are not necessarily ritually abused (Ellason, Ross & Fuchs, 1996). Many ritual abuse victims also claim to have had paranormal experiences, such as astral travel, out-of-body, and near-death experiences, in which their spirits left their physical body.
Many of these spiritual beliefs may be viewed by secular clinicians as unusual or extreme, but would not be so-viewed in many mainstream religions. The less traditional beliefs are consistent with the spiritual practices of many alternative religions. Studies in mainstream psychology are finding high rates of paranormal experience in the general population. Van Lommel, van Wees, Meyers, and Elfferich (2001) found that of 344 cardiac arrest patients resuscitated after being clinically dead, 62 (18%) reported near-death experiences involving a “special state of consciousness”, including specific elements such as out-of-body experience, pleasant feelings, moving through a tunnel, communication with light, deceased relatives, or a life review. Greyson (2000) found that people who believed they had left their physical bodies in close brushes with death reported more dissociative symptoms than people without such experiences, but that their level of symptoms was significantly lower than patients with pathological dissociative disorders. Ross and Joshi (1992) found the incidence of 65.7% of paranormal experience in the general population. The most common were deja vu (54.6%), precognitive dreams (17.8%), and mental telepathy (15.6%).
Possession phenomena are not restricted to patients with histories of ritual abuse, nor are they necessarily associated with a psychiatric disorder. Possession phenomena have a higher incidence in cultures with beliefs in spirits or evil, such as some rural Asian cultures (Chiu, 2000). The DSM-IV acknowledges that nonpathological possession trance states are common within certain cultures and religions, within its discussion of Dissociative Trance Disorder (a proposed diagnostic category for further study, pp. 727-729).
The spiritual beliefs of ritual abuse victims’ are directly derived from years of inculcation in the doctrines and practices of Satanism and abusive witchcraft, generally including the formative years of early childhood, and often under the tutelage of their parents. Victims’ spiritual beliefs must be interpreted within this cultural context.
Wolfgang G. Jilek (2001), Past Chairman, Transcultural Psychiatry Section of the World Psychiatric Association, explains that many psychological conditions are actually "Culture-bound Reactive Syndromes". For instance, he reports that persecutory delusions and auditory hallucinations are not necessarily indicative of Schizophrenia in persons of African cultural background and that acute transient psychotic reactions occur especially frequently in African and Afro-Caribbean populations. He reports that increasingly, the French term bouffée délirante, introduced by Magnan in 1886, is being used to designate these transient psychotic or psychosis-like reactions. He writes (bold italics added for emphasis, spelling unchanged from the original):
The bouffée délirante reactions are sudden attacks of brief duration with paranoid delusions and often concomitant hallucinations, typically precipitated by an intense fear of magical persecution through sorcery or witchcraft. They are also characterized by a confusional state and by highly emotionalized behaviour and, after the attack, by amnesia, or rather disavowal. In its symptomatology, the bouffée délirante is reminiscent of the transient psychotic reactions occurring in the early phases of industrialization and mass-urbanization in 19th century Europe; described under such names as folie hystérique in Paris and amentia transitonia in Vienna [Morel, 1860; Meymert, 1889]. Indeed, the concept of hysterical psychosis was revived in the 1960s by American psychiatrists with special reference to transient psychotic reactions in non-Western populations [Hollender & Hirsch, 1964; Hirsch & Hollender, 1969], while Swiss psychiatrists during the same period introduced the label "emotional psychosis" for bouffée délirante-like reactions triggered by the fear of witchcraft, experienced by rural South Italian migrants under acculturation pressure in Swiss cities [Labhardt 1963; Risso & Boeker 1964]. Transient psychotic reactions are of particular interest to comparative cultural psychiatry because they are interwoven with culturally validated beliefs in sorcery and witchcraft which persist, even after the traditional resources of protection from, and of therapeutic action against, the assumed persecution by magical or supernatural powers, are no longer available as a consequence of Westernization and urbanization. While the number of individuals experiencing the pressures of rapid social change is steadily increasing, many feel unprotected against magical forces in which they still firmly believe, and react to acculturation stress with transient psychotic symptom formation.
The implications of Jilek’s thesis for our purpose are clear. Ritual abuse/mind control traumatic stress is a culture-bound condition, uniquely bourne of the subculture of isolation, torture, religious indoctrination, and coercive programming, inherent in ritual trauma and mind control, understandable only in that context, and not to be superimposed onto a model that does not account for its origins, i.e., the diagnostic system of the DSM- IV.
Chart for Differential Diagnosis of Schizophrenia and Ritual Abuse/Mind Control Traumatic Stress
The clinical features that differentiate Ritual abuse/mind control traumatic stress from Schizophrenia are summarized in the attached chart below for easy clinical reference.
This chart draws primarily on the clinical experience of the authors who have treated or assessed a total of 50 patients with ritual abuse and mind control trauma, and hundreds with Schizophrenia, and consultation with other experts in assessment of this population. It also incorporates information drawn from the literature on ritual abuse and mind control trauma; symptomatology related to ritual torture, symbols, artifacts, and holidays; relevant symptoms of the major primary and secondary diagnoses of affected individuals; findings based in psychological assessment of ritual trauma and DID; and research on differential diagnosis of trauma- related disorders from Schizophrenia.
Validation Studies
Two validation studies were performed on these guidelines and chart. A first draft of these were sent to 17 licensed mental health professionals known to have significant knowledge of ritual abuse and/or coercive mind control. They were asked to fill out a short questionnaire about their professional experience and to indicate the degree to which they judged these guidelines to accurately differentiate Schizophrenia from Traumatic Stress from Ritual Abuse or Mind Control. Expertise was defined as a clinician having at least 10 years of licensed clinical experience and as having treated or assessed at least six patients with each disorder.
Thirteen surveys were returned. Three clinicians were judged to have inadequate expertise with at least one of the diagnostic groups. Two did not complete the question about adequate differentiation of the two disorders, but did send an explanation and helpful suggestions for improving the guidelines and chart.
Eight clinicians met criteria for expertise and completed the chart; four psychiatrists, three psychologists and one marriage and family counselor/professional counselor (MFT/PC). Seven of these judged that this chart accurately differentiated 90% to 100% of the patients in each diagnostic group from patients with the other diagnosis. One psychologist judged that it accurately differentiated 90 to 100% of the patients with Traumatic Stress from Ritual Abuse or Mind Control from patients with Schizophrenia, but only about 75% of the patients with Schizophrenia from those with Traumatic Stress from Ritual Abuse or Mind Control.
The second validation study was performed following substantial additions to the article text, and less extensive, but significant additions to the differential diagnosis chart. The newly-revised guidelines and chart were sent to 20 additional licensed mental health professionals known to have experience in ritual abuse and/or coercive mind control. Expertise remained defined as in the first validation study.
Fifteen surveys were returned. Three clinicians had inadequate expertise with one or both diagnostic groups. Twelve clinicians met criteria for expertise and completed the surveys. The study results are as follows:
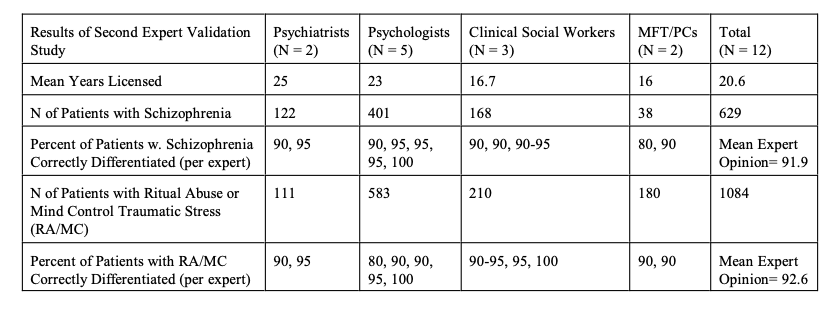
Guidelines to Differential Diagnosis between Schizophrenia and Ritual Abuse/Mind Control Traumatic Stress
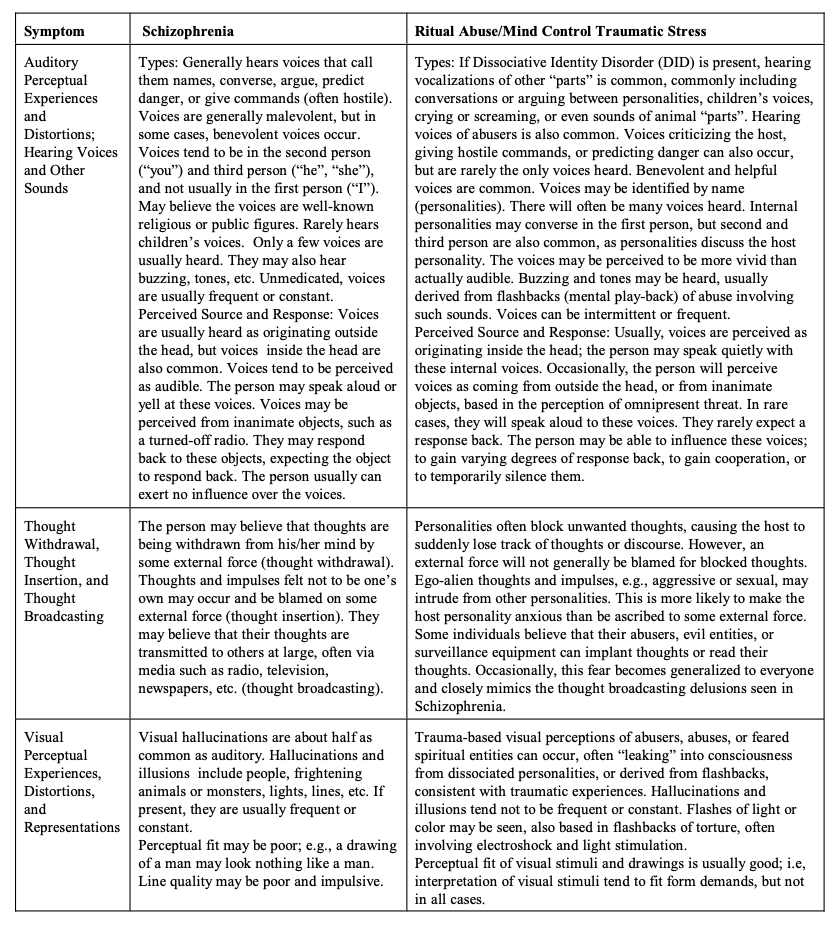
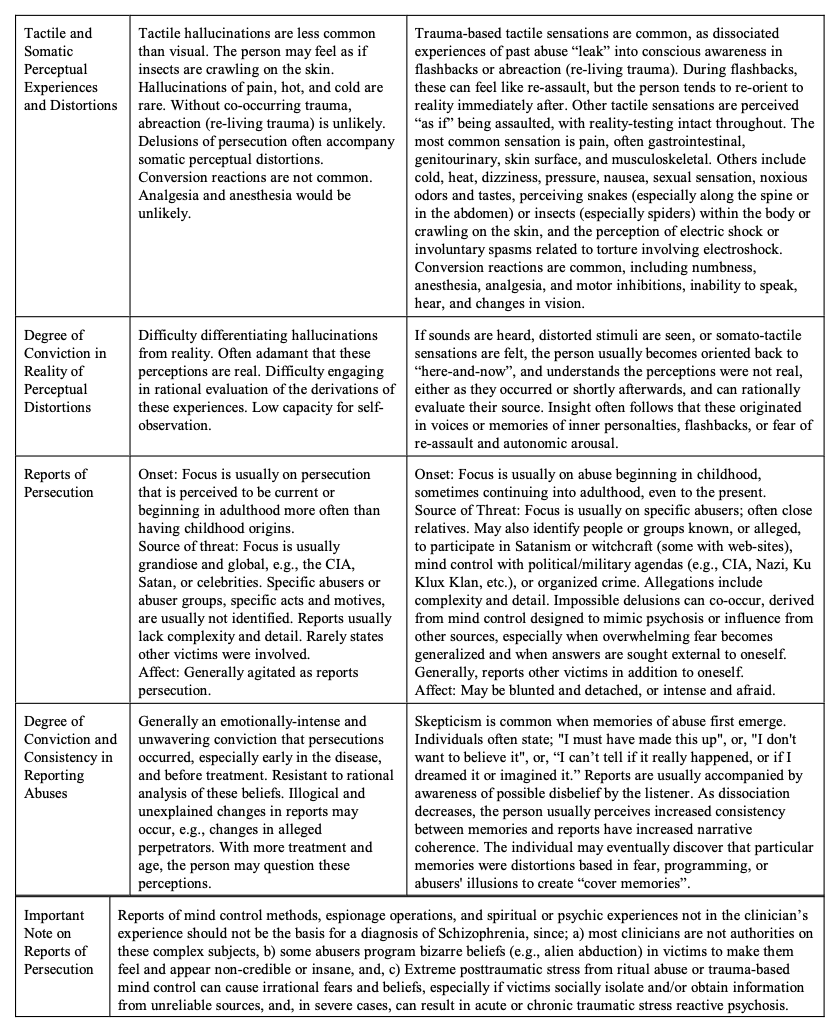
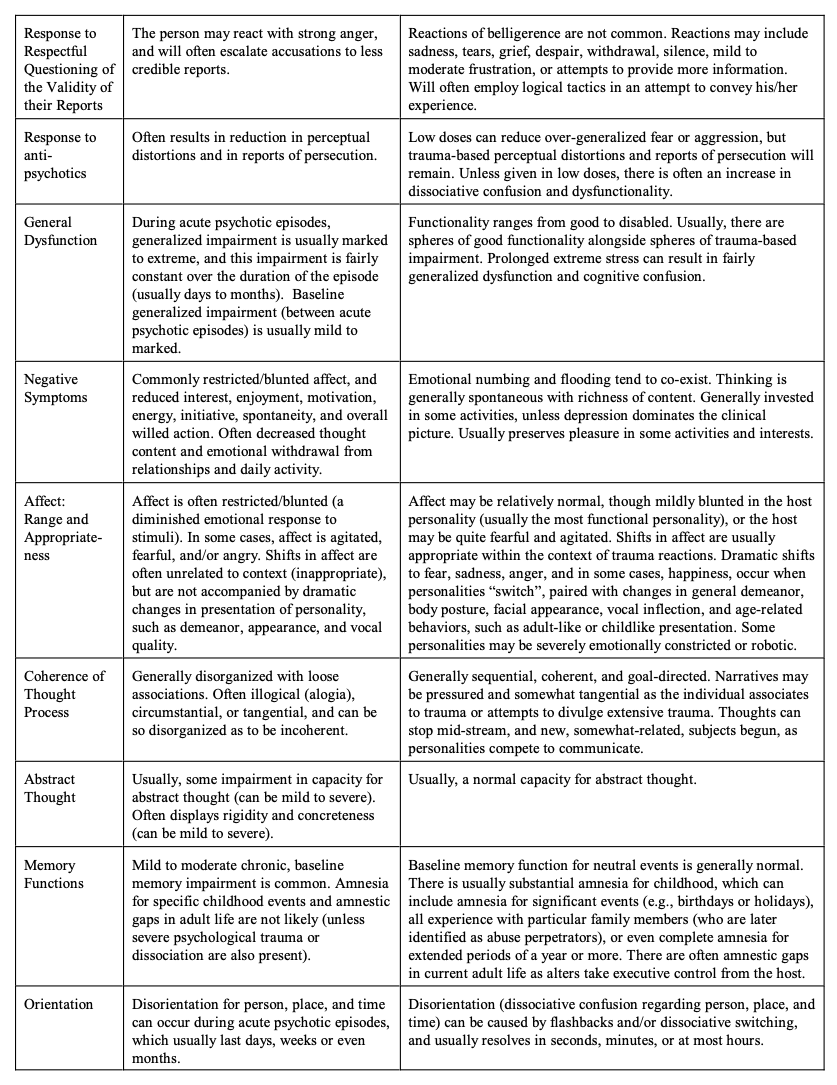
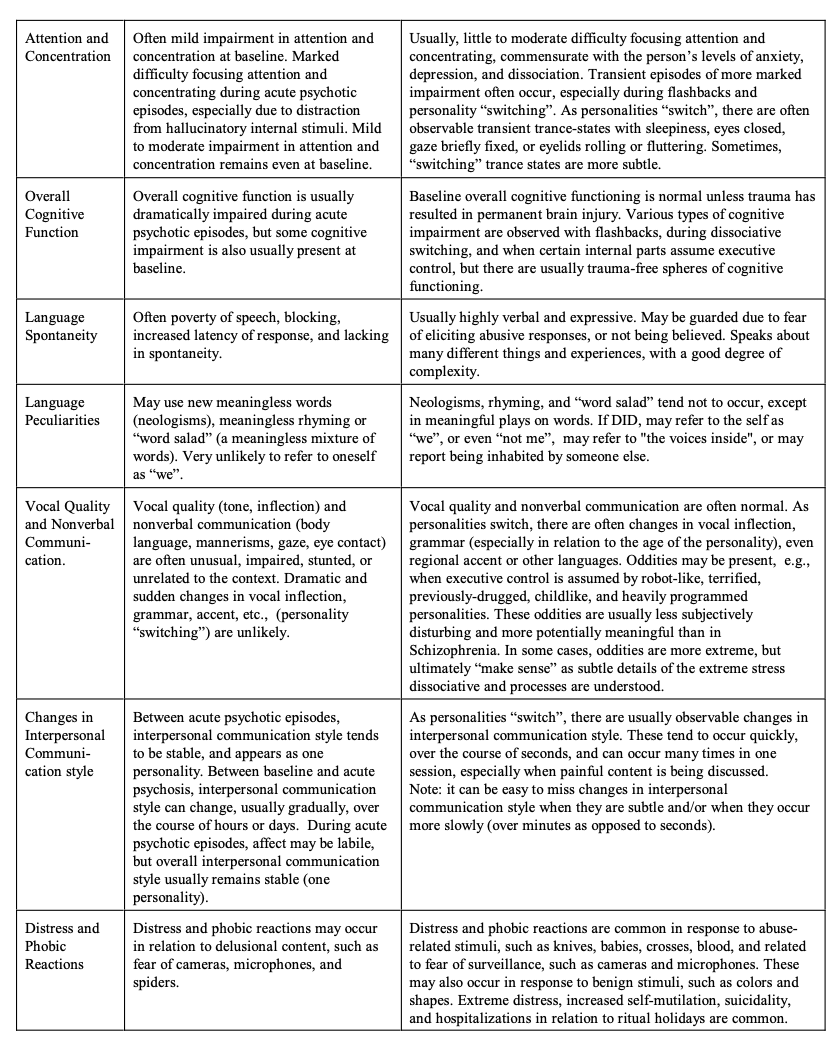
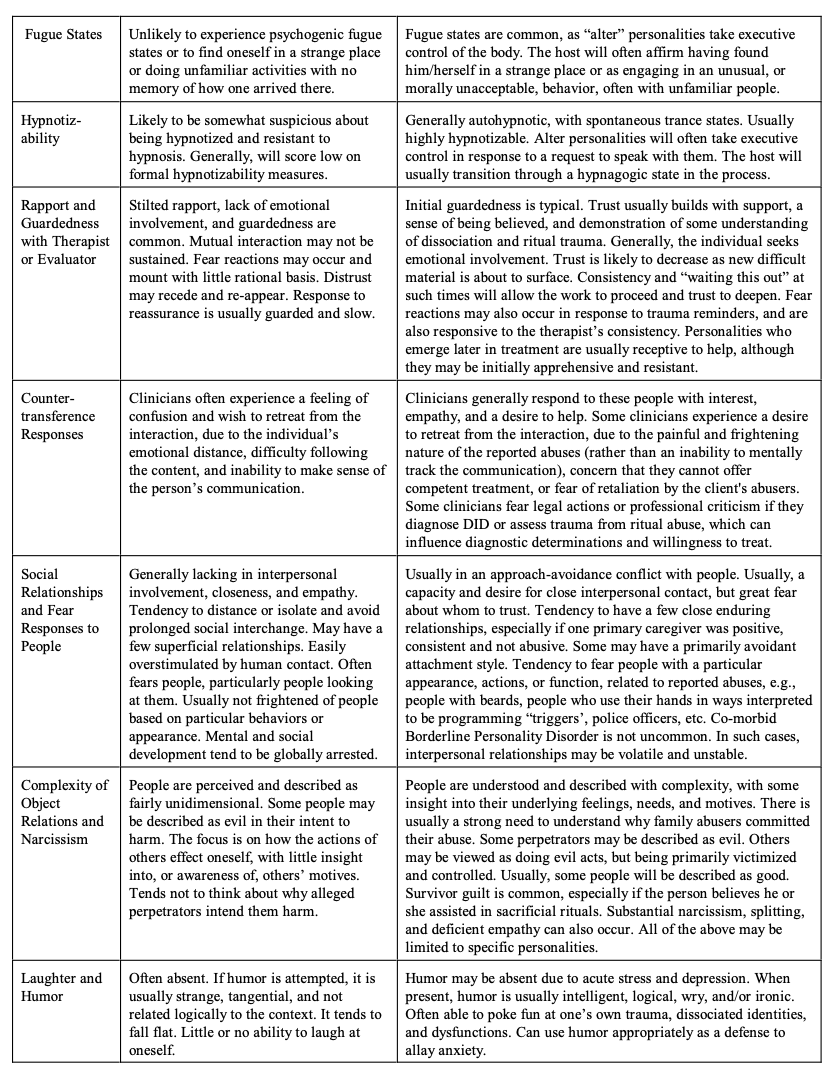
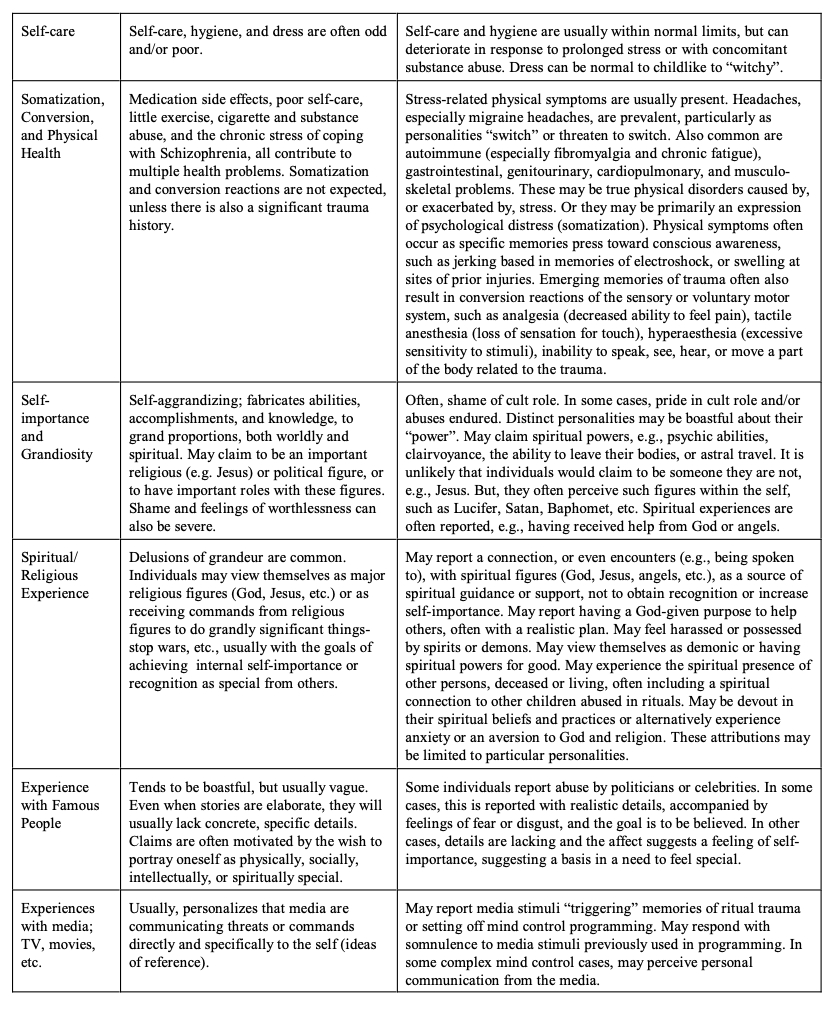
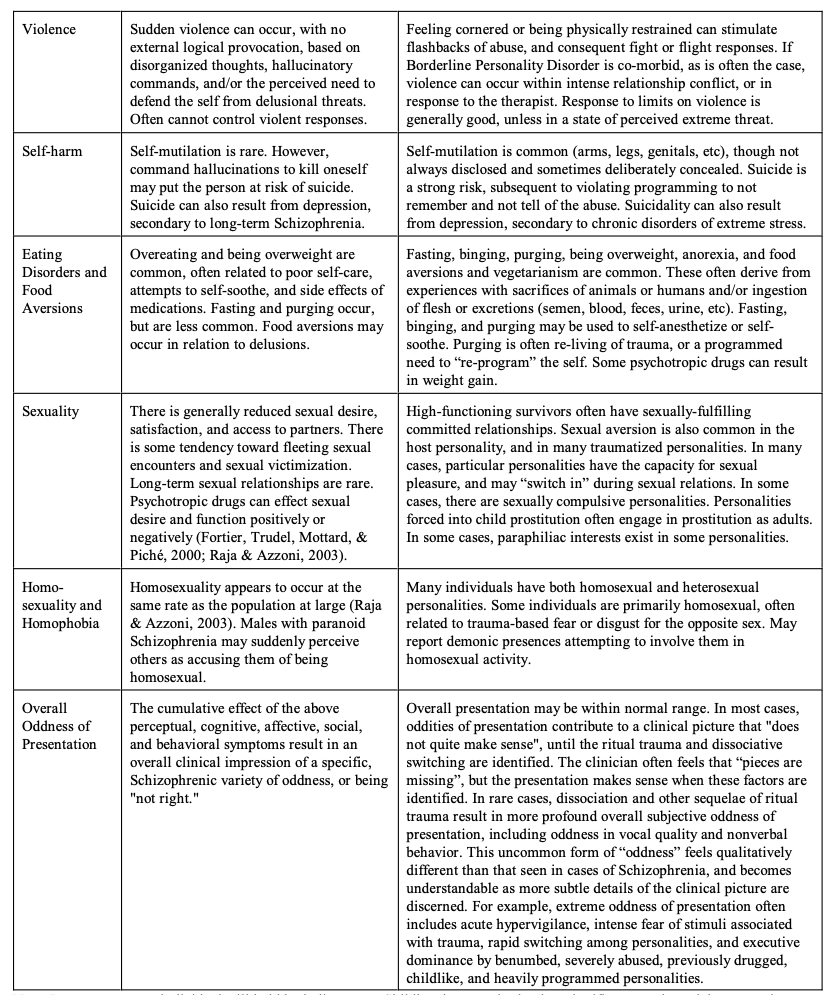
Note: In some cases, an individual will hold both diagnoses. Childhood trauma is clearly a significant psychosocial stressor that may contribute to the neurodevelopment of Schizophrenia. And victims of ritual abuse and mind control are not exempt from the biogenetic determinants that may factor into vulnerability for Schizophrenia.
Conclusion:
These guidelines provide an overview of the complex subjects of ritual abuse and trauma-based mind control, the disorders that frequently result from these abuses, factors that often contribute to the mis-diagnosis of Ritual abuse/mind control traumatic stress as Schizophrenia, and a differential diagnosis chart for easy clinical reference to distinguish between these disorders.
An expert validation study determined that this differential diagnosis chart successfully distinguished between these two populations in most cases. Using this chart, the mean expert opinion was that 91.6% of patients diagnosed with Schizophrenia were successfully differentiated from patients with Ritual abuse/mind control traumatic stress, and that 92% of patients with Ritual abuse/mind control traumatic stress were successfully differentiated from patients diagnosed with Schizophrenia.
In complex cases, it is recommended that clinicians not experienced in ritual abuse and mind control traumatic stress obtain consultation with colleagues with specialized knowledge, in addition to use of the chart, in order to make a differential diagnosis. In rare cases, the diagnostic questions will remain difficult.
It is our hope that these guidelines and chart for differential diagnosis will help diagnosticians recognize and properly diagnose and treat people traumatized by ritual abuse and mind control, and that their frequent mis- diagnosis with Schizophrenia, and the damage that often follows, will one day be a thing of the past.
Bibliography:
American Psychiatric Association (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, D.C.: Author.
Armstrong, J. (1991). The psychological organization of multiple personality disordered patients as revealed on psychological testing. Psychiatric Clinics of North America, 14, 533-546.
Armstrong, J. G., Putnam, F. W., Carlson, E. B., Libero, D. Z., & Smith, S.R. (1997). Development and validation of a measure of adolescent dissociation: The Adolescent Dissociative Experiences Scale. Journal of Nervous & Mental Disease, 185(8), 491-497. The Adolescent Dissociative Experiences Scale is available online, Retrieved November 30, 2003: http://www.energyhealing.net/pdf_files/a-des.pdf.
Armstrong, J.G., & Loewenstein, R.J. (1990). Characteristics of patients with multiple personality and dissociative disorders on psychological testing. Journal of Nervous & Mental Disease, 178(7), 448-454.
Assalian, P., Fraser, R., Tempier, R., & Cohen, D. (2000). Sexuality and quality of life of patients with schizophrenia. International Journal of Psychiatry in Clinical Practice, 4(1), 29-33.
Belitz, J., & Schacht, A. (1992). Satanism as a response to abuse: The dynamics and treatment of Satanic involvement in male youths. Adolescence, 27, 855-872.
Bernet, W., & Chang, D.K. (1997). The differential diagnosis of ritual abuse allegations. Journal of Forensic Science, 42(1), 32-38.
Bliss, E.L. (1980) Multiple personalities: A report of 14 cases with implications for schizophrenia and hysteria. Archives of General Psychiatry, 37 (December), 1388-1397.
Bloom, S.L. (1994) . Hearing the survivor’s voice: Sundering the wall of denial. Journal of Psychohistory, 21(4), 461-477.
Boat, B.W. (1991). Caregivers as surrogate therapists in treatment of a ritualistically abused child. In W.N. Friedrich (Ed.), Casebook of sexual abuse treatment (pp. 1-26). New York: Norton.
Boyd, A. (1991). Blasphemous rumors: Is Satanic ritual abuse fact or fantasy? An investigation. London: HarperCollins.
Braun, B.G. (1986). Treatment of multiple personality disorder. Washington, DC: American Psychiatric Press.
Briere, J. (2002). Multiscale Dissociation Inventory. Odessa , FL : Psychological Assessment Resources.
Brown, D. (1994). Satanic ritual abuse: A therapist's handbook. Denver, CO: Blue Moon Press.
Brown, D., Scheflin, A.W., & Hammond, D.C. (1998). Memory, trauma treatment, and the law: An essential reference on memory for clinicians, researchers, attorneys, and judges. New York: Norton.
Carlson, E.B., & Putnam, F.W. (1993). An update on the dissociative experiences scale. Dissociation, 6, 16-27.
Carlson, E.B., Putnam, F.W., Ross, C.A., Torem, M., Coons, P., Dill, D.L., Loewenstein, R.J., & Braun, B.G. (1993). Validity of the Dissociative Experiences Scale in screening for multiple personality disorder: A multicenter study. American Journal of Psychiatry, 150(7), 1030-1036. The Dissociative Experiences Scale is available on-line; Retrieved November 30, 2003: http://www.energyhealing.net/pdf_files/desii.pdf .
Chiu, S.N. (2000). Historical, religious, and medical perspectives on possession phenomenon. Hong Kong Journal of Psychiatry, 10(1), 14-18.
Chu, J.A., Frey, L.M., Ganzel, B.L., & Matthews, J.A. (1999). Memories of childhood abuse: Dissociation, amnesia, and corroboration. American Journal of Psychiatry, 156(5), 749-755.
Clark, C.M. (1994), Clinical assessment of adolescents involved in Satanism. Adolescence, Summer, XXIV (114), 461-468.
Clay, C. (1996). More Than A Survivor. Saskatoon: University of Saskatchewan Press.Cohen, B.M., & Cox, C.T. (1995). Telling without talking: Art as a window into the world of multiple
personality. New York: Norton.Coleman, J. (1994a). Presenting features in adult victims of Satanist ritual abuse. Child Abuse Review, 3, 83-92.
Coleman, J. (1994b). Satanic cult practices. In V. Sinason (Ed.), Treating survivors of satanic abuse (pp. 242- 253). London, and New York, NY: Routledge.
Comstock, C. (1991). The inner self helper and concepts of inner guidance: Historical antecedents, its role within dissociation, and clinical utilization. Dissociation, 4(3), 165-177.
Comstock, C.M. & Vickery, D. (1992). The therapist as victim: a preliminary discussion. Dissociation, 5(3), 155-158.
Cook, C. (1991). Understanding ritual Abuse: A study of thirty-three ritual abuse survivors. Treating Abuse Today, 1(4), 14-19.
Coons, P.M. (1997). Satanic ritual abuse: First research and therapeutic implications. In G.A. Fraser (Ed.), The dilemma of ritual abuse: Cautions and guides for therapists (pp. 105-117). Washington, DC: American Psychiatric Press.
Cozolino, L. J. (1989). The ritual abuse of children: Implications for clinical practice and research. The Journal of Sex Research, 26 (1), 131-138.
Cozolino, L. J. (1990). Ritualistic child abuse, psychopathology, and evil. Journal of Psychology and Theology, 18 (3), 218-227.
Crabtree, A. (1993). Puzzling over possession: Comments on Dissociation articles on possession, Dissociation, 6(4), 254-259.
Danesino, A., Daniels, J., & McLaughlin, T.J. (1979). Jo-Jo, Josephine, and Joanne: A study of multiple personality by means of the Rorschach test. Journal of Personality Assessment, 43, 300-313.
Daraul, A. (1997) A history of secret societies. Secaucus, Ney Jersey: Citadel Press.Davies, M., Coltheart, M., Langdon, R., & Breen, N. (2002). Monothematic delusions: Towards a two factor
account, Philosophy, Psychiatry & Psychology, 8(2-3), 133-158.DeCamp, J. (1992). The Franklin coverup: Child abuse, Satanism, and murder in Nebraska. Nebraska: AWT.
Dell, P.F. (2004). The subjective/phenomenological concept of Dissociative Identity Disorder. Unpublished manuscript, available from Paul F. Dell, PhD, Trauma Recovery Center 330 W. Brambleton Ave., Suite 206, Norfolk , VA 23510, USA .
De Mause, L. (1994). Why cults terrorize and kill children. The Journal of Psychohistory, 21(4), 505-518. Draijer, N., & Langeland, W. (1999). Childhood trauma and perceived parental dysfunction in the etiology of
dissociative symptoms in psychiatric in-patients. American Journal of Psychiatry, 156(3), 379-385. Driscoll, L. N., & Wright, C. (1991). Survivors of childhood ritual abuse: Multi-generational Satanic cult
involvement. Treating Abuse Today, 1(4), 5-13.Edwards, L. M. (1991). Differentiating between ritual assault and sexual abuse. Journal of Child & Youth Care,
6(4), 169-188.Ehrensaft, D. (1992). Preschool child sex abuse: The aftermath of the Presidio case. The American Journal of
Orthopsychiatry, 62(2), 234-244.Ellason, J.W, & Ross, C.A (1995). Positive and negative symptoms in dissociative identity disorder and
schizophrenia: A comparative analysis. Journal of Nervous & Mental Disease, 183(4), 236-241.Ellason, J.W., Ross, C.A., & Fuchs, D.L. (1995). Assessment of dissociative identity disorder with the Millon
Clinical Multiaxial Inventory-II. Psychological Reports, 76, 895-905.Ellason, J.W., Ross, C.A, & Fuchs, D.L. (1996). Lifetime axis I and II comorbidity and childhood trauma history
in dissociative identity disorder. Psychiatry, 59(3), 255-266.Ellenson, G.S. (1986) Disturbances of perception in adult female incest survivors. Social Casework, March, 149-
159.Emerson, S., & Syron, Y. (1995). Adolescent Satanism: Rebellion masquerading as religion. Counseling &
Values, 39, 145-159.Evers-Szostak, M. & Sanders, S. (1992). The Children's Perceptual Alteration Scale (CPAS): A measure of children's dissociation. Dissociation, 2 (June), 91-98.Exner, J.E. (1978) The Rorschach: A comprehensive system, Volume 2: Current research and advanced
interpretation. New York: Wiley.Fagan, J. & McMahon, P.P. (1984). Incipient multiple personality in children: Four cases. The Journal of
Nervous & Mental Disease, 172(1), 26-36.Faller, K.C. (1994). Ritual abuse: A review of research. APSAC Advisor, 7(1), pp. 1, 19-27.
Feldman, G.C. (1993). Lessons in evil, lessons from the light: A true story of Satanic abuse and spiritual healing. New York: Crown Publishers.
Ferracuti, S., Sacco, R., & Lazzari, R. (1996). Dissociative trance disorder: Clinical and Rorschach findings in ten persons reporting demon possession and treated by exorcism. Journal of Personality Assessment, 66(3), 525- 539.
Fewster, G. (1990). In the shadow of Satan: The ritual abuse of children. Journal of Child and Youth Care Special Issue. Calgary: University of Calgary Press: Calgary
Fine, C. (1989). Treatment errors and iatrogenesis across therapeutic modalities in MPD and allied dissociative disorders. Dissociation, 2(2), 77-82.
Finkelhor, D., Williams, L. M., & Burns, N. (1988). Nursery Crimes. Newbury Park, CA: Sage.Fortier, P., Trudel, G., Mottard J.P., & Piché, L. (2000). The influence of schizophrenia and standard or atypical
neuroleptics on sexual and sociosexual functioning: A review. Sexuality and Disability, 18(2), 85-104.Fraser G. A. (1990). Satanic Ritual Abuse: A cause of multiple personality disorder. Journal of Child & Youth
Care, Special Issue, 55-65.Fraser G. A. (1990). Satanic Ritual Abuse: A cause of multiple personality disorder. Journal of Child & Youth
Care, Special Issue, 55-65.Fraser, G. (1991). The dissociative table technique: a strategy for working with ego states in dissociative
disorders and ego-state therapy. Dissociation, 4(4), 205-213.Fraser, G. (1993a). Special treatment techniques to access the inner personality system of multiple personality
disorder patients. Dissociation, 6(2/3), 193-198.Fraser, G. (1993b). Exorcism rituals: effects on multiple personality disorder patients. Dissociation, 6(4), 239-244.
Fraser, G.A. (1997a). The dilemma of ritual abuse: Cautions and guides for therapists. Washington, D.C.: American Psychiatric Press.
Fraser, G.A. (1997b). Visions of memories: A patient's visual representation of ritual abuse ceremonies. In G.A. Fraser (Ed.), The dilemma of ritual abuse: Cautions and guides for therapists (pp. 183-196). Washington, DC: American Psychiatric Press.
Friesen, J. G. (1991). Uncovering the mystery of MPD. San Bernadino, California: Here's Life Publishing. Friesen, J. G. (1992). Ego-dystonic or ego-alien: Alternate personality or evil spirit? Journal of Psychology &
Theology. 20(3), 197-200.Friesen, J. G. (1993). More than survivors: Conversations with multiple personality clients. San Bernadino,
California: Here's Life Publishing.Frith, C. & Fletcher, P. (1995). Voices From nowhere. Critical Quarterly, 37(2), 71-83.
Gallagher, B. (2001). Assessment and intervention in cases of suspected ritual child sexual abuse. Child Abuse Review, 10, 227-242.
Golston, J. (1993). Ritual abuse: Raising hell in psychotherapy: Creation of cruelty: The political military and multigenerational training of torturers: Violent initiation and the role of traumatic dissociation. Treating Abuse Today, 3(6), 12-19.
Gonzalez, L.S., Waterman, J., Kelly, R.J., McCord, J., & Oliveri, M.K. (1993). Children's patterns of disclosures and recantations of sexual and ritualistic allegations in psychotherapy. Child Abuse & Neglect, 17, 281-289.
Goodman, G.S., Qin, J., Bottoms, B.L., & Shaver (1994). Characteristics and sources of allegations of ritualistic child abuse: Final report to the National Center on Child Abuse and Neglect. [Unpublished manuscript].
Goodman, G. S., Quas, J. A., Bottoms, B. L., Qin, J., Shaver, P. R., Orcutt, H., & Shapiro, C. (1997). Children's religious knowledge: Implications for understanding satanic ritual abuse allegations. Child Abuse & Neglect, 21(11), 1111-1130.
Goodwin, J. (1993). Sadistic abuse: Definition, recognition, and treatment. Dissociation, 6(2/3), 181-187. Goodwin, J.M. (1994). Credibility problems in sadistic abuse. The Journal of Psychohistory, 21(4), 479-496.
Goodwin, J, Hill, S. & Attias, R. (1990). Historical and folk techniques of exorcism: applications to the treatment of dissociative disorders. Dissociation, 3(2), 94-101.
Gould, C. (1992). Diagnosis and treatment of ritually abused children. In D.K. Sakheim & S.E. Devine (Eds.), Out of darkness: Exploring Satanism and ritual abuse (pp. 207-248). New York: Lexington Books.
Gould, C. (1995). Denying ritual abuse of children. Journal of Psychohistory, 22(3), 329-339.Gould, C., & Cozolino, L. (1992). Ritual abuse, multiplicity, and mind-control. Journal of Psychology and
Theology, 20(3), 194-196.Gould, C., & Graham-Costain, V. (1994). Play therapy with ritually abused children. Treating Abuse Today,
4(2), 4-1; 4(3), 14-19.
Gould, C., & Neswald, D. (1992). Basic treatment and program neutralization strategies for adult MPD survivors of satanic ritual abuse. Treating Abuse Today, 2(3), 5--10.
Graves, S.M. (1989). Dissociative disorders and dissociative symptoms at a community mental health center.Dissociation, 2(3), 119-127.
Greaves, G. B. (1992). Alternative hypotheses regarding claims of satanic cult activity. A critical analysis. In D. K. Sakheim, & S. F. Devine, (Eds.), Out of darkness: Exploring Satanism and ritual abuse. (pp. 45-72). New York: Lexington Books.
Greyson, B. (2000). Dissociation in people who have near-death experiences: Out of their bodies or out of their minds. The Lancet, 355, 460-463.
Groenendijk, I. & van der Hart, O. (1995). Treatment of DID and DDNOS patients in a regional institute for ambulatory mental health care in the Netherlands: a survey. Dissociation, 8(2), 73-83.
Hammond, D. C. (1992). Hypnosis in MPD: Ritual abuse (also known as The Greenbaum speech), Fourth Annual Eastern Regional Conference on Abuse and Multiple Personality. Retrieved February 21, 2003:http://home.att.net/~mcra/green.htm .
Hartman, C.R. & Burgess, A.W. (1993). Information processing of trauma. Child Abuse and Neglect, 17(1), 47- 58.
Harvey, S. (1993). Ann: Dynamic play therapy with ritual abuse. In T. Kottman & C. Schaefer, C. (Eds.). Play therapy in action: A casebook for practitioners (pp. 371-415). Northvale, New Jersey: Aronson..
Hassan, S. (1990). Combating cult mind control. Rochester, VT: Park Street Press.Hassan, S. (2000). Releasing the bonds: Empowering people to think for themselves. Danbury, CT : Aitan Publishing.
Hendrickson, K., McCarty, T., & Goodwin, J. (1990). Animal Alters: A Case Report. Dissociation, 3(4), 218 ̄221.
Hersha, L., Hersha, C., Griffis, D., & Schwarz, T. (2001). Secret weapons: Two sister’s terrifying true story of sex, spies, and sabotage. Far Hills, New Jersey: New Horizon Press.
Hill, S., & Goodwin, J. (1989). Satanism; Similarities between patient accounts and pre-Inquisition historical sources. Dissociation, 2(1), 39-44.
Hirsch, S.J., & Hollender, M.H. (1969). Hysterical psychosis: Clarification of the concept. American Journal of Psychiatry, 125, 909-915
Hollender, M.H., & Hirsch, S.J. (1964). Hysterical psychosis. American Journal of Psychiatry, 120, 1066-1074. Hornstein, N.L. (1993). Recognition and differential diagnosis of dissociative disorders in children and
adolescents. Dissociation, 6(2/3), 136-144.Hudson, P.S. (1990). Ritual child abuse: A survey of symptoms and allegations. Journal of Child and Youth
Care, Special issue: In the shadow of Satan: The ritual abuse of children, 27-54.
Hudson, P.S. (1991). Ritual child abuse: discovery, diagnosis and treatment. Saratoga, CA: R & E Publishers. Ireland, S.J., & Ireland, M..J. (1994). A case history of family and cult abuse. The Journal of Psychohistory,
21(4), 417-428.
Jilek, W.G. (2001). Cultural factors in psychiatric disorders. Paper presented at the 26th Congress of the World Federation for Mental Health, July 2001. Available on-line. Retrieved December 12, 2003:http://www.mentalhealth.com/mag1/wolfgang.html .
Johnson, M. (1994). Fear and power: From naivete to a believer in cult abuse. The Journal of Psychohistory, 21(4), 435-441.
Jones, D.P.H. (1991). Ritualism and child sexual abuse. Child Abuse & Neglect, 15, 163-170.Jonker, F., & Jonker-Bakker, P. (1991). Experiences with ritualistic child sexual abuse: A case study from the
Netherlands. Child Abuse & Neglect, 15(3), 191-196.Jonker, F, & Jonker-Bakker, I. (1997). Effects of Ritual Abuse: The results of three surveys in the Netherlands.
Child Abuse & Neglect, 21(6) 541-556.Katchen, M. (1992). The history of Satanic religions. In D. K. Sakheim, & S. F. Devine, (Eds.), Out of
Darkness: Exploring Satanism and Ritual Abuse (pp. 1-19). New York: Lexington Books.Katchen, M., & Sakheim, D. (1992). Satanic beliefs and practices. In D. K. Sakheim, & S. F. Devine, (Eds.),
Out of Darkness: Exploring Satanism and Ritual Abuse. (pp. 21-43). New York: Lexington Books.
Keane, T.M., Malloy, P.F., & Fairbank, J.A. (1984). The empirical development of an MMPI-subscale for the assessment of combat-related Posttraumatic Stress Disorders. Journal of Consulting & Clinical Psychology, 52, 888-891.
Keith, J. (1998). Mind control, world control. Kempton, IL: Adventures Unlimited Press.Kelley, S.J. (1989). Stress responses of children to sexual abuse and ritualistic abuse in day-care centers. Journal
of Interpersonal Violence, 4(4), 501-513.King, G. F., & Yorker, B. (1996). Case studies of children presenting with a history of ritualistic abuse. Journal of Child & Adolescent Psychiatric Nursing, 9(2), 18-26.
Kinscherff, R., & Barnum, R (1992). Child forensic evaluation and claims of ritual abuse or Satanic cult activity: A critical analysis. In D.K. & S.E. Devine (Eds.), Out of Darkness: Exploring Satanism and ritual abuse (pp. 73-107). New York, NY: Lexington Books.
Kluft, R. P. (1987). First-rank symptoms as a diagnostic clue to multiple personality disorder. American Journal of Psychiatry, 144(3), 293-298.
Kluft, R.P. (1988). The phenomenology and treatment of extremely complex multiple personality disorder. Dissociation, 1(4), 47-58.
Kluft, R.P. (1989a). Iatrogenic creation of new alter personalities. Dissociation, 2(2), 83-91.Kluft, R. P. (1989b). Editorial : Reflections on allegation of ritual abuse. Dissociation, 2(4), 191-193.
Kluft, R.P. (1994). Treatment trajectories in multiple personality disorder. Dissociation, 7(1), 63-76. Kluft, R. P. (1995). Six completed suicides in dissociative identity disorder patients: Clinical observations.
Dissociation, 8(2), 104-111.Labhardt, F. (1963). Die schizophrenieahnlichen Emofionspsychosen, Berlin: Springer.
Labott, S.M., Leavitt, F., Braun, B.G., & Sachs, R.A. (1992). Rorschach indicators of multiple personality disorder. Perceptual & Motor Skills, 75, 147-158.
Labott, S.M., & Wallach, H.R. (2002). Malingering dissociative identity disorder: Objective and projective assessment. Psychological Reports, 90, 525-538.
Lawrence, K.J., Cozolino, L., & Foy, D.W. (1995). Psychological sequelae in adult females reporting childhood ritualistic abuse. Child Abuse and Neglect, 19(8), 975-984.
Leavitt, F. (1994). Clinical correlates of alleged Satanic abuse and less controversial sexual molestation. Child Abuse & Neglect, 18(4), 387-392.
Leavitt, F. (2000a). Texture response patterns associated with sexual trauma of childhood and adult onset: Developmental and recovered memory implications. Child Abuse & Neglect, 24(2), 251-257.
Leavitt, F. (2000b). Surviving roots of trauma: Prevalence of silent signs of sex abuse in patients who recover memories of childhood sex abuse as adults. Journal of Personality Assessment, 74(2), 311-323.
Leavitt F., & Labott, S. M.(1998a). Revision of the Word Association Test for assessing associations of patients reporting Satanic ritual abuse in childhood. Journal of Clinical Psychology, 54(7), 933-943.
Leavitt F., & Labott, S. M.(1998b). Rorschach indicators of dissociative identity disorder: Clinical utility and theoretical implications. Journal of Clinical Psychology, 54(6), 803-810.
Leavitt, F., & Labott, S.M. (2000). The role of media and hospital exposure on Rorschach response patterns by patients reporting satanic ritual abuse. American Journal of Forensic Psychology, 18(2), 35-55.
Lloyd, D. W. (1992). Ritual child abuse: Definitions and assumptions. Journal of Child Sexual Abuse, 1(3), 1-14.
Lockwood, C. (1993) Other altars: Roots and realities of cultic and Satanic ritual abuse and multiple personality disorder. Minneapolis, MN: Compcare.
Lotto, D. (1994). On witches and witch hunts: Ritual and Satanic cult abuse. The Journal of Psychohistory, 21(4), 373-396.
Lovitt, R., & Lefkoff, G. (1985). Understanding multiple personality disorder with the Comprehensive Rorschach System. Journal of Personality Assessment, 49, 289-294.
Luxenberg, T., Spinazzola, J., &. van der Kolk, B. (2001). Complex trauma and Disorders of Extreme Stress (DESNOS): Diagnosis, part one: Assessment. Directions in Psychiatry (21), Retrieved August 24, 2003:http://www.traumacenter.org/webarticles.html .
Luxenberg, T., Spinazzola, J., Hidalgo, J., Hunt, C., &. van der Kolk, B. (2001), Complex trauma and Disorders of Extreme Stress (DESNOS) Diagnosis, part two: Treatment. Directions in Psychiatry (21), Retrieved August 24, 2003: http://www.traumacenter.org/webarticles.html .
Macfarland, R.B.,& Lockerbie, G. (1994). Difficulties in treating ritually abused children. Journal of Psychohistory, 21(4), 429-434.
MacHovec, F. (1992). Cults: Forensics and therapeutic aspects. Behavior Sciences and the Law, 10, 31-37. Magnan, V. (1886). cK. Ey. H., Bernard, P., & Brisset, C. (1963). Manuel de Psychiatrie. 2nd.rev.edn. Masson:
Paris., p. 245.Mandell, H. E., & Schiff, M.(1993). Schizophrenia or terrifying reality? A supervisor's dilemma. The Clinical
Supervisor, 11(20), 127-133.Mangen, R. (1992). Psychological testing and ritual abuse. In D.K. Sakheim & S.E. Devine (Eds.), Out of
darkness: Exploring Satanism and ritual abuse (pp. 147-173). New York: Lexington.Marks, J. (1979). The Search for the Manchurian Candidate: The CIA and mind control. New York: Times
Books.
Mayer, R.S. (1991). Satan's Children: Case studies in multiple personality. New York: Putnam.
McCulley, D. (1994). Satanic ritual abuse: A question of memory. Psychology & Theology, 22(3), 167-172.
McFarland, R. B. & Lockerbie, G. (1994). Difficulties in treating ritually abused children. The Journal of Psychohistory, 21(4), 429-434
McFadyen, A., Hanks, H. & James, C. (1993). Ritual abuse: A definition. Child Abuse Review, 2, 35-41. Meynert, T.(1889). Amentia, die VerwirrtheK. Jahrbuch der Psychiatrie (Vienna) 9, 1 -112.
Moise, J., & Leichner, P. (1996). Prevalence of dissociative symptoms and disorders within an adult outpatient population with schizophrenia. Dissociation, IX(3), 190-196.
Moore, M.S. (1994). Common characteristics in the drawings of ritually abused children and adults. In V. Sinason (Ed.), Treating survivors of satanic abuse (pp. 221-241). London, and NY, NY: Routledge.
Morel, B.A. (1860). Traife des maladies menfales. Masson: Paris.Moriarty, A. R. (1991). Adolescent Satanic cult dabblers: A differential diagnosis. Journal of Mental Health
Counseling, 13(3), 393--404.Moriarty, A. (1992) The psychology of adolescent Satanism: A guide for parents, counselors, clergy, and
teachers. Westport, CT: Praeger Publishers/Greenwood.Mueser, K.T. & Butler, R.W. (1987). Auditory hallucinations in combat-related chronic posttraumatic stress
disorder. American Journal of Psychiatry, 144(3), 299-302.Murphy, P.E (1994). Dissociative experiences and dissociative disorders in a non-clinical university student group. Dissociation, 7(1), 28-34.
Neswald, D., & Gould, C. (1993). Basic treatment and program neutralization strategies for adult MPD Survivors of Satanic ritual abuse. Treating Abuse Today, 4 (3), 14-19.
Neswald, D., Gould, C., & Graham-Costain, V. (1991).“Common “programs” observed in survivors of Satanic ritual abuse. The California Therapist, 3(5), 47– 50.
Nijenhuis, E.R.S. (2000). Somatoform dissociation: Major symptoms of dissociative disorders. Journal of Trauma & Dissociation, 1(4), 7-32. The Somatoform Dissociation Questionnaire (SDQ-20) is available on-line; Retrieved November 30, 2003: http://www.psychotherapist.org/Sdq20.PDF.
Noblitt, J.R. (1995). Psychometric measures of trauma among psychiatric patients reporting ritual abuse. Psychological Reports, 77(3), 743-747.
Noblitt, J.R., & Perskin, P. (2000). Cult and ritual Abuse: Its history, anthropology, and recent discovery in contemporary America; Revised edition. Westport, CT: Praeger Publishers.
Nurcombe, B., & Unutzer, J (1991). The ritual abuse of children: clinical features and diagnostic reasoning. Journal of the American Academy of Child and Adolescent Psychiatry, 30(2), 272-276.
Ogawa, J.R., Sroufe, A., Weinfield, N.S., Carlson, E.A., & Egeland, B. (1997). Development and the fragmented self: Longitudinal study of dissociative symptomatology in a nonclinical sample. Development & Psychopathology, 9, 855-879.
Oksana, C. (1994, revised 2001). Safe passage to healing: A guide for survivors of ritual abuse. NY: Harper Perennial.
Paley, K.S. (1992). Dream wars: a case study of a woman with multiple personality disorder. Dissociation, 5(2), 111-116.
Pelcovitz D., van der Kolk, B.A., Roth S., Mandel, F., Kaplan, S., & Resicket, P. (1997). Development of a criteria set and a structured interview for disorder of extreme stress (SIDES). Journal of Traumatic Stress,10(1), 3–16.
Perlman, S. D. (1995). One analyst's journey into darkness: Countertransference resistance to recognizing sexual abuse, ritual abuse, and multiple personality disorders. Journal of the American Academy of Psychoanalysis, 23(1), 137-51.
Peterson, G. (1991). Children coping with trauma: Diagnosis of "dissociation identity disorder". Dissociation Progress in the Dissociative Disorders, 4(3), 152-164.
Peterson, G. (1996). Treatment of early onset. In J.L. Spira & I.D. Yalom (Eds.), Treating Dissociative Identity Disorder (pp. 135-181). San Francisco: Josey-Bass.
Pulling, P., & Cawthorn, K. (1989). The devil’s web: Who is stalking your children for Satan?. Lafayette, Louisiana: Huntington House.
Putnam, F.W. (1997). Dissociation in children and adolescents: A developmental perspective. New York: Guilford Press.
Putnam, F. W., Helmers, K., & Trickett, P. K. (1993). Development, reliability and validity of a child dissociation scale. Child Abuse & Neglect, 17, 731-742. The Child Dissociative Checklist is available on-line; Retrieved November 30, 2003: http://www.energyhealing.net/pdf_files/cdc.pdf .
Putnam, F.W., Helmers, K., Horowitz, L.A., & Trickett, P.K. (1995). Hypnotizability and dissociativity in sexually abused girls, Child Abuse & Neglect, 19(5), 645-655.
Pynoos, R.S., Steinberg, A.M., & Goenjian, A. (1996). Traumatic stress in childhood and adolescence: Recent developments and current controversies. In B.A. van der Kolk, A.C. McFarlane, & L. Weisaeth (Eds.). Traumatic stress: The effects of overwhelming experience on mind, body, and society (pp 331-358). New York: Guilford Press.
Raja, M. & Azzoni, A. (1998). Long-Term atypical psychoses. German Journal of Psychiatry, 1(1), 34-48. Raja, M. & Azzoni, A. (2003). Sexual behavior and sexual problems among patients with severe chronic
psychoses. Europea Psychiatry, 18, 70-76.Raschke, C.A. (1990). Painted black: From drug killings to heavy metal : the alarming true story of how
Satanism is terrorizing our communities. New York: Harper and Row.
Read, J., Agar, K., Argyle, N., & Aderhold, V. (2003). Sexual and physical abuse in childhood and adulthood as predictors of hallucinations, delusions and thought disorder. Psychology & Psychotherapy: Theory, Research and Practice, 76, 1-22.
Read, J., & Argyle, N. (1999). Hallucinations, delusions, and thought disorder among adult psychiatric inpatients with a history of child abuse. Psychiatric Services, 50, 1467-147
Read, J., Perry, B., Moskowitz, A., & Connolly, J. (2001). The contribution of early traumatic events to schizophrenia in some patients: A traumagenic neurodevelopmental model. Psychiatry: Interpersonal & Biological Processes, 64 (4). Retrieved August 24, 2003: http://www.childtrauma.org/CTAMATERIALS/Psychiatry_02.pdf .
Rhue, J., Lynn, S., & Sandberg, D. (1995). Dissociation, imagination and fantasy in childhood: A comparison of physically, sexually, and non-abused children. Contemporary Hypnosis, 12, 131-136.
Riley, K. C. (1988). Measurement of dissociation. Journal of Nervous & Mental Disease, 176, 449–450. Risso, M., & Boker, W. (1964). Verhexangswahn. Karger. New York: Basel - (Bibliotheca Psychiatrica et
Neurologica 124)
Rockwell, R.B. (1994). One psychiatrist’s view of Satanic ritual abuse. The Journal of Psychohistory, 21(4), 443-460.
Rockwell, R.B. (1995). Insidious deception. The Journal of Psychohistory, 22(3), 312-328.Rose, E. (1996). Reaching for the light: A guide for ritual abuse survivors and Their therapists. Cleveland:
Pilgrim Press.Rosik, C.H. (2003). Critical issues in the dissociative disorders field: Six perspectives from religiously sensitive practitioners. Journal of Psychology & Theology, 31(2), 113-128.
Ross, C.A. (1989). Multiple personality disorder: Diagnosis, clinical features, and treatment. New York: Wiley.
Ross, C.A. (1995). Satanic ritual abuse: Principles of treatment. Toronto: University of Toronto Press.
Ross, C. A. (1997). Dissociative identity disorder: Diagnosis, clinical features and treatment of multiple personality (2nd ed.). New York: Wiley. The Dissociative Disorders Interview Schedule- DSM-IV Version is also available on-line; Retrieved November 30, 2003: http://www.rossinst.com/dddquest.htm.
Ross, C.A. (2000). Bluebird : Deliberate creation of Multiple Personality by psychiatrists. Manitou, Canada: Manitou Communications
Ross, C.A., Fast, E., Anderson, G., Auty, A., & Todd, J. (1990). Somatic symptoms in multiple sclerosis and MPD, Dissociation, 3(2),102-106.
Ross, C.A., & Joshi, S. (1992). Paranormal experiences in the general population. Journal of Nervous & Mental Diseases, 180, 356-360.
Ross, C.A., Miller, S.D., Bjornson, L., Reagor, P., Fraser, G.A., & Anderson, G. (1990). Schneiderian symptoms in multiple personality disorder and schizophrenia. Comprehensive Psychiatry, 31(2), 111-118..
Ross. C.A., Miller, S.D., Reagor, P., Bjornson, L., Fraser, G.A., & Anderson, G. (1990). Schneiderian symptoms in multiple personality disorder and schizophrenia. Comprehensive Psychiatry, 31(2), 111-118.
Rutz, C. (2001). A nation betrayed: The chilling and true story of secret cold war experiments performed on our children and other innocent people. Grass Lake, MI: Fidelity Publishing.
Ryder, D., & Noland, J.T. (1992). Breaking the circle of Satanic ritual abuse: Recognizing and recovering from the hidden trauma. Minneapolis, MN: CompCare Publishers.
Ryder, D. (1997). Cover-up of the century: Satanic ritual crime and world conspiracy. Ohio: CSS Publishing. Sacco, M.L., & Farber, B.A. (1999). Reality testing in adult women who report childhood sexual and physical
abuse. Child Abuse & Neglect, 23(11), 1193-1203.Sachs, R.G. (1990). The role of sex and pregnancy in Satanic cults. Journal of Prenatal & Perinatal Psychology
& Health, 5 (2), 105-114Sakheim, D.K. (1996). Clinical aspects of sadistic ritual abuse. In L.K. Michelson & W.J. Ray (Eds), Handbook
of dissociation: Theoretical, empirical, and clinical perspectives, (pp. 569-594). New York: Plenum Press. Sakheim, D.K., & Devine, S.E. (Eds.) (1992). Out of darkness: Exploring Satanism and ritual abuse. New York: Lexington.
Sar, V., Kundakci, T., Kiziltan, E., Bakim, B., & Bozkurt, O. (2000). Differentiating dissociative disorders from other diagnostic groups through somatoform symptoms in Turkey. Journal of Trauma and Dissociation, 1(4), 67-80.
Scaer, R. (2001). The body bears the burden: Trauma, dissociation, and disease. New York: Haworth
Schlenger, W.E., & Kulka, R.A. (1989). PTSD scale development for the MMPI-2. Research Triangle Park: Research Triangle Institute.
Scott, S. (2001). The politics and experience of ritual abuse: Beyond disbelief. Philadelphia: Open University Press.
Scroppo, J. C., Drob, S.L., Weinberger, J.L., & Eagle, P. (1998). Identifying dissociative identity disorder: A self-report and projective study. Journal of Abnormal Psychology, 107(2) 272-284.
Sheflin, A. & Opton, E. (1978). The mind manipulators. New York: Grosset & Dunlap.Silberg, J. L. (1998). Dissociative symptomatology in children and adolescents as displayed on psychological testing. Journal of Personality Assessment, 71(3), 421-39.
Sinason, V. (1994). Treating survivors of satanic abuse. London, and NY, NY: Routledge.
Sinason, V. (2005). Just like others, satanists abuse. Community Care, 5-11 May, p. 18.
Smith, C. (1998). The Magic Castle. New York: St. Martin's Press.
Smith, M. (1993). Ritual Abuse: What it is, why it happens, how to help. San Francisco: Harper.
Smith, M.R. (1992). A reply to Ganaway: the problem of using screen memories as an explanatory device in accounts of ritual abuse. Dissociation, 5(2), 117-119.
Smith, M., & Pazder, L. (1981). Michelle Remembers. New York: Pocket Books.Snow B., & Sorensen (1990). Ritualistic child abuse in a neighborhood setting. Journal of Interpersonal
Violence, 5(4), 474-487.Stafford, L. L. (1993). Dissociation and multiple personality disorder: A challenge for psychosocial nurses.
Journal of Psychosocial Nursing & Mental Health Services, 31(1), 15-20.Steele, H. (2003). Unrelenting catastrophic trauma within the family: When every secure base is abusive.
Attachment and Human Development, 5(4), 353-366.Steele, K. H. (1989). A model for abreaction with MPD and other dissociative disorders. Dissociation, 2(2/3), 151-159.
Steinberg, M. (1996). The psychological assessment of dissociation. In L.K. Michelson & W.J. Ray (Eds), Handbook of dissociation: Theoretical, empirical, and clinical perspectives (pp. 251-267). New York: Plenum Press.
Steinberg, M., Cicchetti, D.V., Buchanan, J., Rakfeldt, J., & Rounsaville, B (1994). Distinguishing between multiple personality disorder (dissociative identity disorder) and schizophrenia using the structured clinical interview for DSM-IV dissociative disorders. Journal of Nervous & Mental Disease, 182(9), 495-502.
Stratford, L. (1993). Satan's Underground. Gretna, LA: Pelican Publishing.
Summit, R.C. (1994). The dark tunnels of McMartin. The Journal of Psychohistory, 21(4), 397-416.
Tamarkin, C. (1994a). Investigative Issues in Ritual Abuse Cases, Part I. Treating Abuse Today, 4 (4), 14-23.
Tamarkin, C. (1994b). Investigative Issues in Ritual Abuse Cases, Part II. Treating Abuse Today, 4 (5), 5-9. Tate, T. (1991). Children for the devil: Ritual abuse and Satanic crime. London: Methuen.
Tutkun, H., Yargic, L.I., & Sar, V. (1996). Dissociative identity disorder presenting as hysterical psychosis. Dissociation, 9, 244-252.
Uherek, A.M. (1991). Treatment of a ritually abused preschooler. In W.N. Friedrich (Ed.) Casebook of sexual abuse treatment (pp. 70-92). New York: Norton.
Valente SM. (1992). The challenge of ritualistic child abuse. Journal of Child & Adolescent Psychiatric Mental Health Nursing, 5(2), 37-46.
Valente SM. (2000). Controversies and challenges of ritual child abuse. Journal of Psychosocial Nursing & Mental Health Services, 38(11), 8-17.
van Benschoten, S.C. (1990). Multiple Personality Disorder and Satanic ritual abuse: The Issue of credibility.Dissociation, 3(1), 22-30.
van der Hart, O. (1993). Multiple personality disorder in Europe: Impressions. Dissociation, 6(2/3), 102-118.
van der Kolk (1996). The body keeps the score: Memory and the evolving psychobiology of post traumatic stress. In B. Van der Kolk, A. C. McFarlane, & L. Weisaeth (Eds.), Traumatic stress: The effects of overwhelming experience on mind, body, and society (pp. 214-241). New York: Guilford.
van der Kolk, B.A., McFarlane, A.C., & Weisaeth, L. (1996). Traumatic stress: The effects of overwhelming experience on mind, body, and society. New York: Guilford.
van der Kolk B.A., Roth S., Pelcovitz D., & Mandel F. (1993). Complex PTSD: Results of the PTSD field trial for DSM-IV. Washington, DC: American Psychiatric Association.
van Lommel, P., van Wees, R., Meyers, V., & Elfferich, I. (2001). Near-death experience in survivors of cardiac arrest: A prospective study in the Netherlands. Lancet, 358(9298), 2039-2045.
Vanderlinden, J., Van Dyck, R., Vandereycken, W., Vertommen, H., & Verkes, R.J. (1993). The Dissociation Questionnaire (DIS-Q): Development and characteristics of a new self-report questionnaire. Clinical Psychology and Psychotherapy, 1, 21-27.
Vesper, J.H. (1991). The use of healing ceremonies in the treatment of multiple personality disorder. Dissociation, 4(2), 109-114.
Wagner, E.E., & Heise, M.R. (1974). A comparison of Rorschach records of three multiple personalities. Journal of Personality Assessment, 38(4), 308-331.
Wagner, E., Allison, R., & Wagner, A. (1983). Diagnosing multiple personalities with the Rorschach: A confirmation. Journal of Personality Assessment, 47, 143-149.
Waller, G., Hamilton, K., Elliott, P., Lewendon, J., Stopa, L., Waters, A., Kennedy, F., Lee, G., Pearson, D., Kennerley, H., Hargreaves, I., Bashford, V., & Chalkley, J. (2000). Somatoform dissociation, psychological dissociation, and specific forms of trauma. Journal of Trauma & Dissociation, 1, 81-98.
Waterman, J., Kelly, R.J., Olivieri, M.K., & McCord, J. (1993). Beyond the playground walls: Sexual abuse in preschools. New York: Guilford.
Weinstein, H. (1990). Psychiatry and the CIA: Victims of mind control. Washington, DC: American Psychiatric Press.
Weir, I.K., & Wheatcroft, M.S. (1995). Allegations of children's involvement in ritual sexual abuse: Clinical experience of 20 cases. Child Abuse & Neglect, 19(4), 491-505.
Welburn, K. R., Fraser, G. A., Jordan, S. A., Cameron, C., Webb, L. M., & Raine, D. (2003). Discriminating Dissociative Identity Disorder from Schizophrenia and feigned dissociation on psychological tests and structured interview. Journal of Trauma & Dissociation, 4(2), 109-130.
Whitfield, C.L., Silberg, J., & Fink, P.J. (2002). Misinformation concerning child sexual abuse and adult survivors. New York: Haworth Press.
Williams, M.B (1991). Clinical work with families of MPD patients: assessment and issues for practice, Dissociation, 4(2), 92-98.
Wong, B., & McKeen, J. (1990). A case of multiple life-threatening illnesses related to early ritual abuse. Journal of Child & Youth Care, Special Issue: In the shadow of Satan: The ritual abuse of children, 1-26.
Woodsum, G.M. (1998). The ultimate challenge: A revolutionary, Sane and sensible response to ritualistic and cult-related abuse. WY: Action Resources International
Young, W.C. (1992). Recognition and treatment of survivors reporting ritual abuse. In D.K. Sakheim & S.E. Devine (Eds.), Out of darkness: Exploring Satanism and ritual abuse (pp. 249-278). New York: Lexington.
Young, W. C. (1993). Sadistic ritual abuse. An overview in detection and management. Primary Care, 20(2), 447-458.
Young, W.C., Sachs, R.G., Braun, B.G., & Watkins, R.T. (1991). Patients reporting ritual abuse in childhood: A clinical syndrome. Report of 37 cases. Child Abuse and Neglect, 15, 181-189.
Young, G.R., Wagner, E.E., & Finn, R.F. (1994).A comparison of three Rorschach diagnostic systems and use of the Hand Test for detecting multiple personality disorder in outpatients. Journal of Personality Assessment, 62(3), 485-497.
Young, W.C., & Young, L.J. (1997). Recognition and special treatment issues in patients reporting childhood sadistic ritual abuse. In G.A. Fraser (Ed.), The dilemma of ritual abuse: Cautions and guides for therapists (pp. 65-103). Washington, DC: American Psychiatric Press.
Youngson, S.C. (1993). Ritual abuse: Consequences for professionals. Child Abuse Review, 2, 251-262.